

Effect of allopurinol in chronic kidney disease progression and cardiovascular risk
- PMID: 20538833
- PMCID: PMC2924417
- DOI: 10.2215/CJN.01580210
Effect of allopurinol in chronic kidney disease progression and cardiovascular risk
Abstract
Background and objectives: Hyperuricemia is associated with hypertension, inflammation, renal disease progression, and cardiovascular disease. However, no data are available regarding the effect of allopurinol in patients with chronic kidney disease.
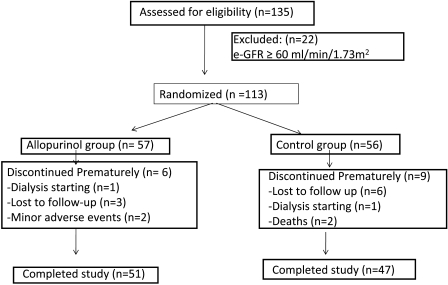
Design, setting, participants, & measurements: We conducted a prospective, randomized trial of 113 patients with estimated GFR (eGFR) <60 ml/min. Patients were randomly assigned to treatment with allopurinol 100 mg/d (n = 57) or to continue the usual therapy (n = 56). Clinical, biochemical, and inflammatory parameters were measured at baseline and at 6, 12, and 24 months of treatment. The objectives of study were: (1) renal disease progression; (2) cardiovascular events; and (3) hospitalizations of any causes.
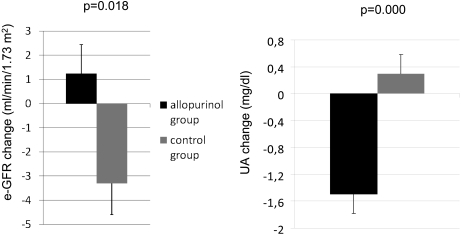
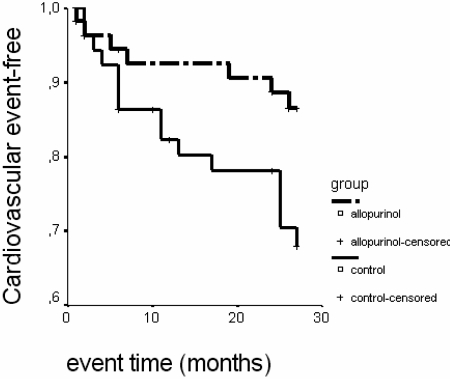
Results: Serum uric acid and C-reactive protein levels were significantly decreased in subjects treated with allopurinol. In the control group, eGFR decreased 3.3 +/- 1.2 ml/min per 1.73 m(2), and in the allopurinol group, eGFR increased 1.3 +/- 1.3 ml/min per 1.73 m(2) after 24 months. Allopurinol treatment slowed down renal disease progression independently of age, gender, diabetes, C-reactive protein, albuminuria, and renin-angiotensin system blockers use. After a mean follow-up time of 23.4 +/- 7.8 months, 22 patients suffered a cardiovascular event. Diabetes mellitus, previous coronary heart disease, and C-reactive protein levels increased cardiovascular risk. Allopurinol treatment reduces risk of cardiovascular events in 71% compared with standard therapy.
Conclusions: Allopurinol decreases C-reactive protein and slows down the progression of renal disease in patients with chronic kidney disease. In addition, allopurinol reduces cardiovascular and hospitalization risk in these subjects.
Figures
Comment in
-
Risk factors: Does uric acid level affect renal and cardiovascular risk?Nat Rev Nephrol. 2010 Oct;6(10):562. doi: 10.1038/nrneph.2010.118. Nat Rev Nephrol. 2010. PMID: 20886678 No abstract available.
-
Allopurinol verbessert Prognose bei Patienten mit chronischer Nierenerkrankung.Praxis (Bern 1994). 2011 Mar 16;100(6):373-4. doi: 10.1024/1661-8157/a000469. Praxis (Bern 1994). 2011. PMID: 21412750 German. No abstract available.
References
-
- Edwards NL: The role of hyperuricemia and gout in kidney and cardiovascular disease. Clev Clin J Med suppl 5: S13–S16, 2008 - PubMed
-
- Gagliardi A, Miname M, Santos R: Uric acid: A marker of increased cardiovascular risk. Atherosclerosis 202: 11–17, 2009 - PubMed
-
- Johnson RJ, Kang DH, Feig D, Kivlighn S, Kanellis J, Watanabe S, Tuttle KR, Rodriguez-Iturbe B, Herrera-Acosta J, Mazzali M: Is there a pathogenetic role for uric acid in hypertension and cardiovascular and renal disease? Hypertension 41: 1183–1190, 2003 - PubMed
-
- Suliman ME, Johnson RJ, Garcia-Lopez E, Qureshi AR, Molinaei H, Carrero JJ, Heimbürger O, Bárány P, Axelsson J, Lindholm B, Stenvinkel P: J-shaped mortality relationship for uric acid in CKD. Am J Kidney Dis 48: 761–771, 2008 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
