

Renal function and healthcare costs in patients with polycystic kidney disease
- PMID: 20538839
- PMCID: PMC2924421
- DOI: 10.2215/CJN.00780110
Renal function and healthcare costs in patients with polycystic kidney disease
Abstract
Background and objectives: Characterizing relationships of kidney function to healthcare costs in polycystic kidney disease has applications for economic evaluations of standard and emerging therapies.
Design, setting, participants, & measurements: The administrative records (2003 to 2006) of a private health insurer were examined to identify polycystic kidney disease patients (n = 1913) from ICD9 diagnosis codes on billing claims. The first available diagnostic claim was assumed as an index date, and baseline estimated GFR (eGFR) was computed using closest serum creatinine value. The associations of eGFR with annualized charges were modeled by nonlinear and linear regression.
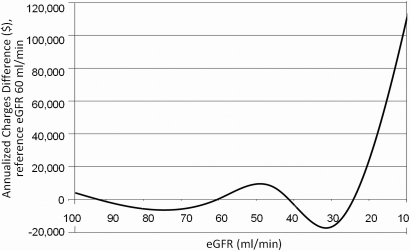
Results: Medical, pharmacy, and total healthcare costs varied significantly by baseline kidney function, such that mean total annualized charges (unadjusted) were approximately 5-fold higher in patients with eGFR < 15 ml/min compared with those with eGFR >or= 90 ml/min. After adjustment for age and gender, total charges did not differ significantly among patients with eGFR > 30 ml/min, and but rose precipitously with eGFR < 30 ml/min. Each ml/min decline <30 ml/min predicted approximately $5435 higher adjusted annual charges. Results were similar after adjustment for baseline diabetes and cardiovascular disease as identified in claims, while significantly higher adjusted charges were detected with eGFR = 31 to 60 ml/min versus >or=90 ml/min in a subgroup free of diabetes and cardiovascular disease.
Conclusions: Healthcare charges are associated with advanced renal dysfunction in polycystic kidney disease patients. Strategies that prevent loss of renal function below 30 ml/min have the potential to generate substantial reductions in medical charges.
Figures
References
-
- Grantham J, Cowley BJ, Torres VE: Progression of autosomal dominant polycystic kidney disease (ADPKD) to renal failure. In: The Kidney: Physiology and Pathophysiology, edited by Seldin DW, Geibisch G, Philadelphia, Lippincott Williams and Wilkins, 2000, pp 2513–2536
-
- Grantham JJ, Torres VE, Chapman AB, Guay-Woodford LM, Bae KT, King BF, Jr., Wetzel LH, Baumgarten DA, Kenney PJ, Harris PC, Klahr S, Bennett WM, Hirschman GN, Meyers CM, Zhang X, Zhu F, Miller JP: Volume progression in polycystic kidney disease. N Engl J Med 354: 2122–2130, 2006 - PubMed
-
- Bear JC, McManamon P, Morgan J, Payne RH, Lewis H, Gault MH, Churchill DN: Age at clinical onset and at ultrasonographic detection of adult polycystic kidney disease: Data for genetic counselling. Am J Med Genet 18: 45–53, 1984 - PubMed
-
- Churchill DN, Bear JC, Morgan J, Payne RH, McManamon PJ, Gault MH: Prognosis of adult onset polycystic kidney disease re-evaluated. Kidney Int 26: 190–193, 1984 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
