

Perfusion scintigraphy and patient selection for lung volume reduction surgery
- PMID: 20538961
- PMCID: PMC2970864
- DOI: 10.1164/rccm.201001-0043OC
Perfusion scintigraphy and patient selection for lung volume reduction surgery
Abstract
Rationale: It is unclear if lung perfusion can predict response to lung volume reduction surgery (LVRS).
Objectives: To study the role of perfusion scintigraphy in patient selection for LVRS.
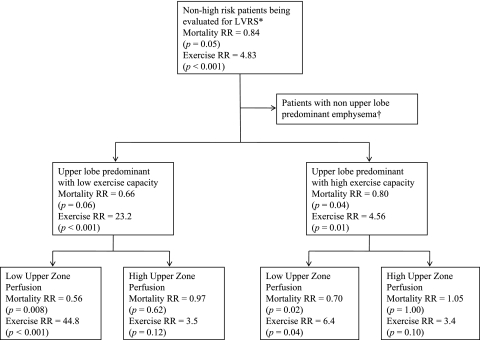
Methods: We performed an intention-to-treat analysis of 1,045 of 1,218 patients enrolled in the National Emphysema Treatment Trial who were non-high risk for LVRS and had complete perfusion scintigraphy results at baseline. The median follow-up was 6.0 years. Patients were classified as having upper or non-upper lobe-predominant emphysema on visual examination of the chest computed tomography and high or low exercise capacity on cardiopulmonary exercise testing at baseline. Low upper zone perfusion was defined as less than 20% of total lung perfusion distributed to the upper third of both lungs as measured on perfusion scintigraphy.
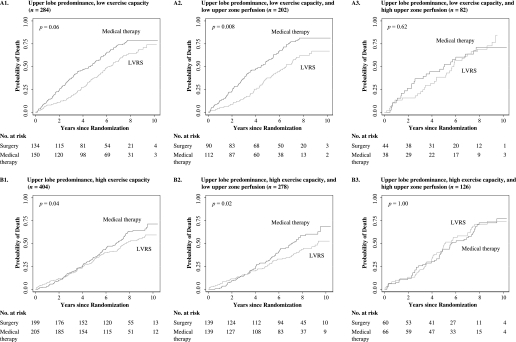
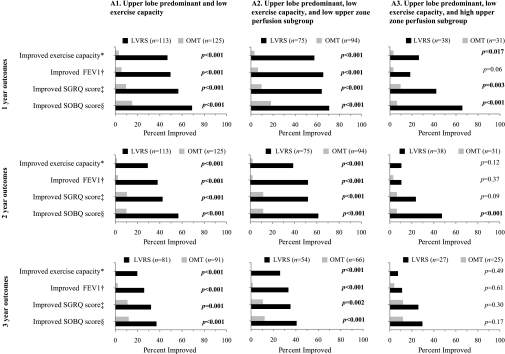
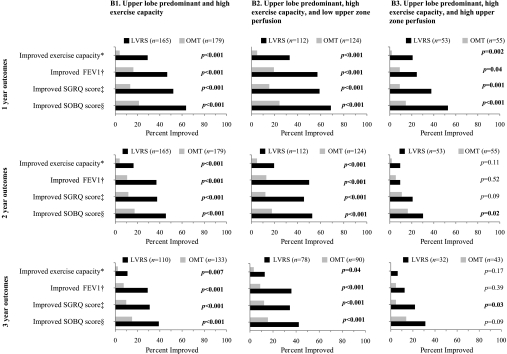
Measurements and main results: Among 284 of 1,045 patients with upper lobe-predominant emphysema and low exercise capacity at baseline, the 202 with low upper zone perfusion had lower mortality with LVRS versus medical management (risk ratio [RR], 0.56; P = 0.008) unlike the remaining 82 with high perfusion where mortality was unchanged (RR, 0.97; P = 0.62). Similarly, among 404 of 1,045 patients with upper lobe-predominant emphysema and high exercise capacity, the 278 with low upper zone perfusion had lower mortality with LVRS (RR, 0.70; P = 0.02) unlike the remaining 126 with high perfusion (RR, 1.05; P = 1.00). Among the 357 patients with non-upper lobe-predominant emphysema (75 with low and 282 with high exercise capacity) there was no improvement in survival with LVRS and measurement of upper zone perfusion did not contribute new prognostic information.
Conclusions: Compared with optimal medical management, LVRS reduces mortality in patients with upper lobe-predominant emphysema when there is low rather than high perfusion to the upper lung.
Figures
References
-
- Fishman A, Martinez F, Naunheim K, Piantadosi S, Wise R, Ries A, Weinmann G, Wood DE. A randomized trial comparing lung-volume-reduction surgery with medical therapy for severe emphysema. N Engl J Med 2003;348:2059–2073. - PubMed
-
- Thurnheer R, Engel H, Weder W, Stammberger U, Laube I, Russi EW, Bloch KE. Role of lung perfusion scintigraphy in relation to chest computed tomography and pulmonary function in the evaluation of candidates for lung volume reduction surgery. Am J Respir Crit Care Med 1999;159:301–310. - PubMed
-
- Berger RL, Wood KA, Cabral HJ, Goodnight-White S, Ingenito EP, Gray A, Miller J, Springmeyer SC. Lung volume reduction surgery: a meta-analysis of randomized clinical trials. Treat Respir Med 2005;4:201–209. - PubMed
-
- Chenuel B, Haouzi P, Olivier P, Marie PY, Chalon B, Borrelly J. Effect of exercise on lung-perfusion scanning in patients with bronchogenic carcinoma. Eur Respir J 2002;20:710–716. - PubMed
Publication types
MeSH terms
Grants and funding
- N01HR76113/HR/NHLBI NIH HHS/United States
- N01HR76107/HR/NHLBI NIH HHS/United States
- N01HR76102/HR/NHLBI NIH HHS/United States
- N01HR76104/HR/NHLBI NIH HHS/United States
- N01HR76118/HR/NHLBI NIH HHS/United States
- N01HR76115/HR/NHLBI NIH HHS/United States
- N01HR76105/HR/NHLBI NIH HHS/United States
- N01HR76111/HR/NHLBI NIH HHS/United States
- N01HR76114/HR/NHLBI NIH HHS/United States
- N01HR76103/HR/NHLBI NIH HHS/United States
- N01HR76110/HR/NHLBI NIH HHS/United States
- N01HR76119/HR/NHLBI NIH HHS/United States
- N01HR76108/HR/NHLBI NIH HHS/United States
- N01HR76117/HR/NHLBI NIH HHS/United States
- N01HR76106/HR/NHLBI NIH HHS/United States
- N01HR76109/HR/NHLBI NIH HHS/United States
- 1K23HL089353-01A1/HL/NHLBI NIH HHS/United States
- N01HR76116/HR/NHLBI NIH HHS/United States
- N01HR76112/HR/NHLBI NIH HHS/United States
- N01HR76101/HR/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
