

Effects of recession versus tenotomy surgery without recession in adult rabbit extraocular muscle
- PMID: 20538996
- PMCID: PMC3061502
- DOI: 10.1167/iovs.10-5523
Effects of recession versus tenotomy surgery without recession in adult rabbit extraocular muscle
Abstract
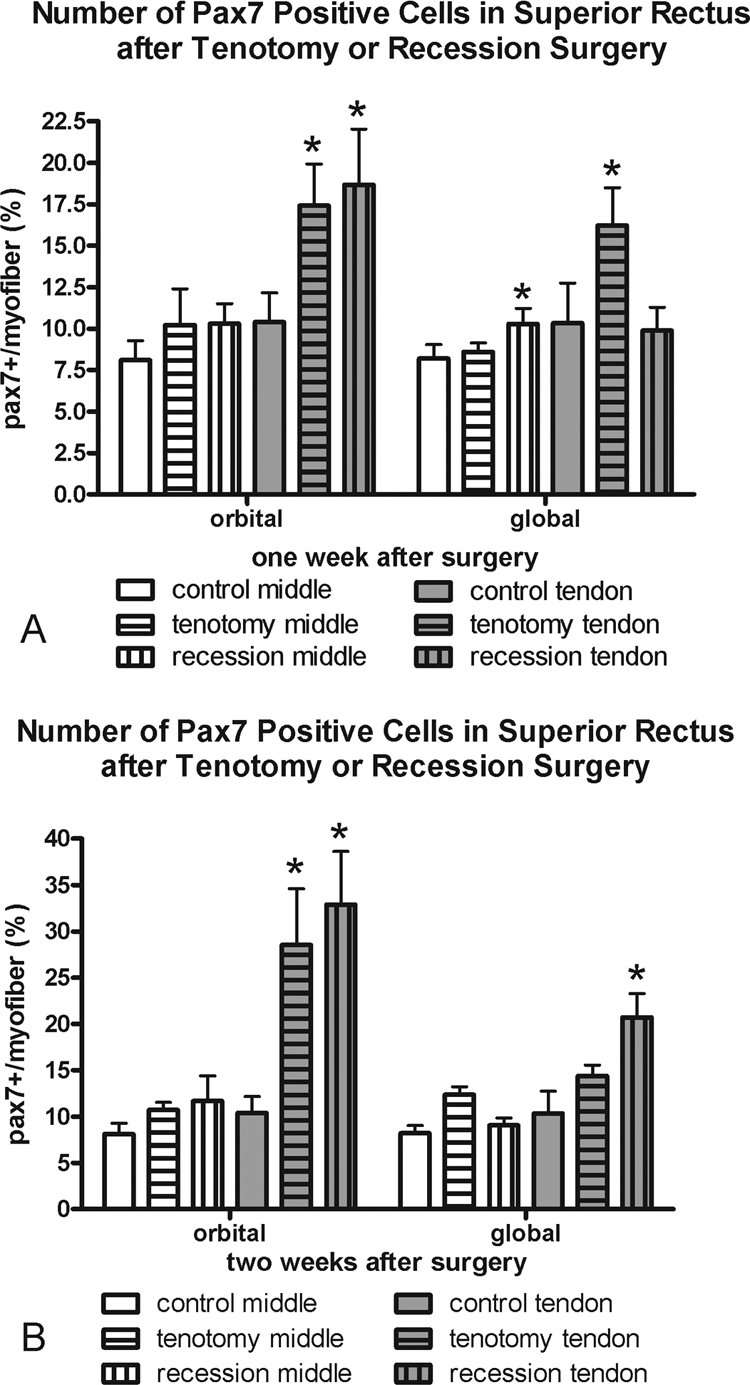
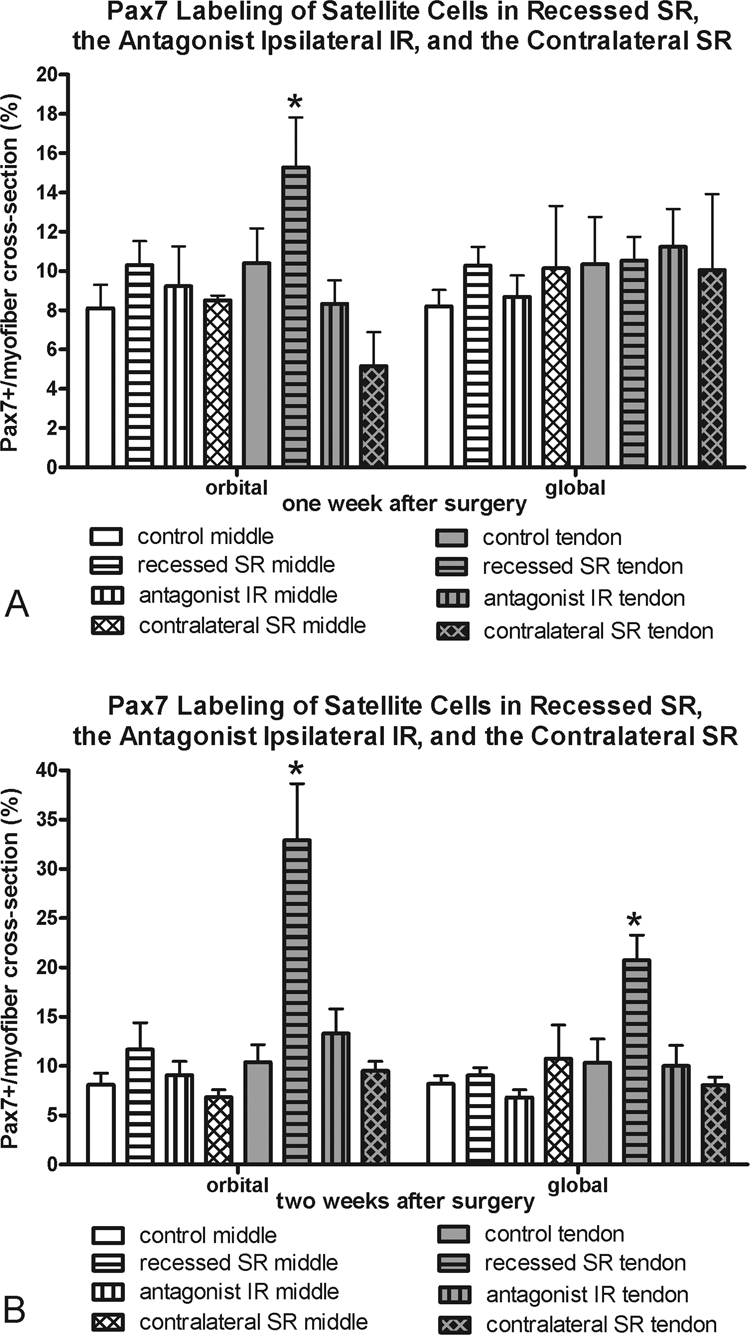
Purpose: Surgical recession of an extraocular muscle (EOM) posterior to its original insertion is a common form of strabismus surgery, weakening the rotational force exerted by the muscle on the globe and improving eye alignment. The purpose of this study was to assess myosin heavy chain (MyHC) isoform expression and satellite cell activity as defined by Pax7 expression in recessed EOMs of adult rabbits compared with that in muscles tenotomized but not recessed and with that in normal control muscles.
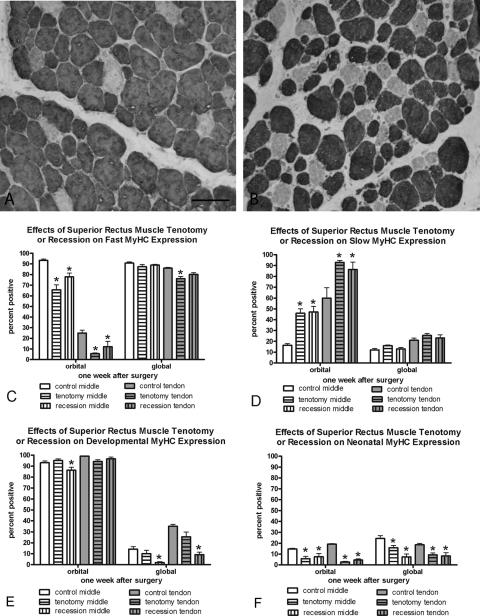
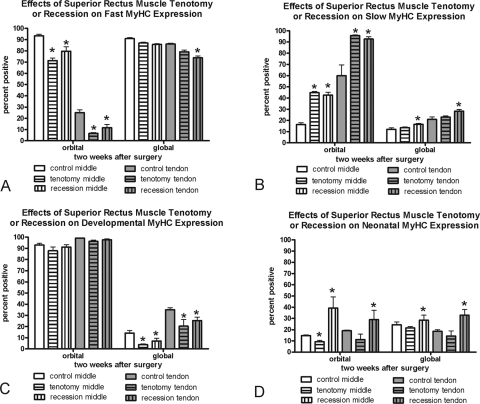
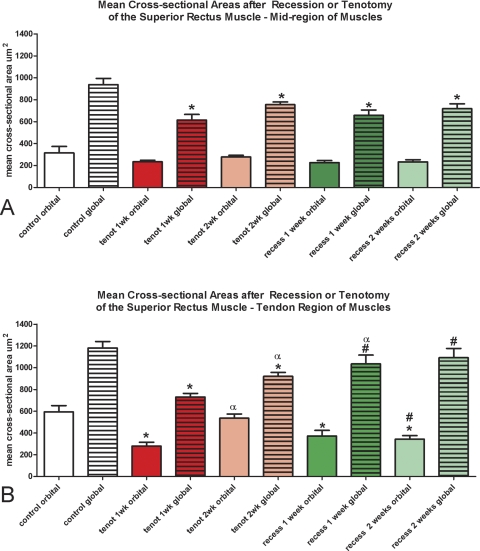
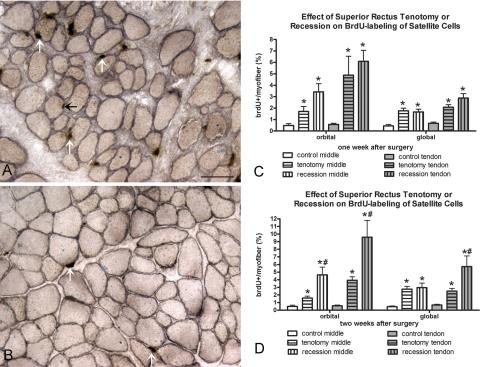
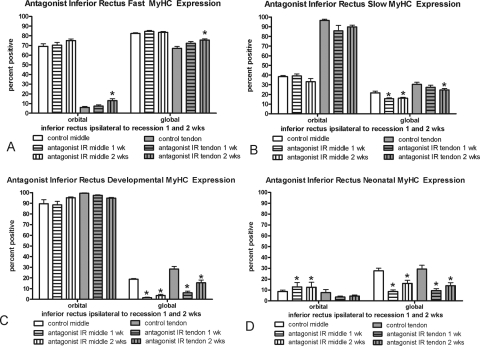
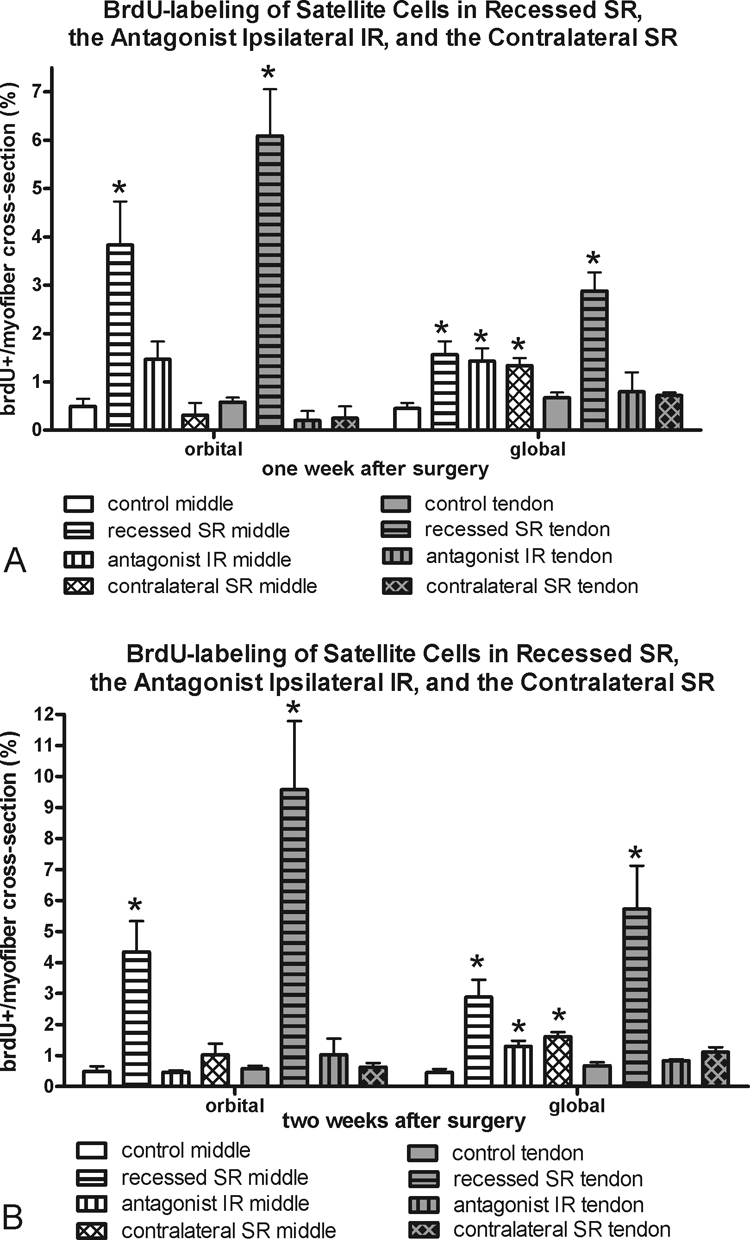
Methods: The scleral insertion of the superior rectus muscle was detached and sutured either 7 mm posterior to its original insertion site (recession surgery) or at the same site (tenotomy). One day before euthanization, the rabbits received bromodeoxyuridine (BrdU) injections. After 7 and 14 days, selected EOMs from both orbits were examined for changes in fast, slow, neonatal, and developmental MyHC isoform expression, Pax7 expression, and BrdU incorporation.
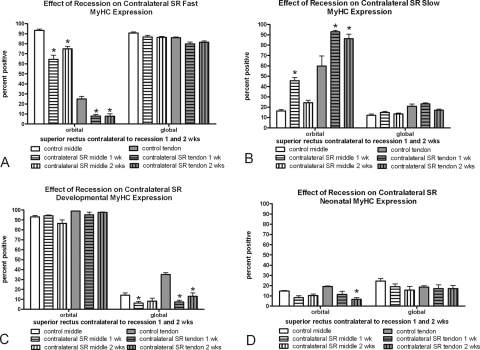
Results: Recession and tenotomy surgery resulted in similar changes in the surgical EOMs. These included a decreased proportion of fast MyHC myofibers, an increased proportion of slow MyHC myofibers, and increased BrdU-positive satellite cells. Similar changes were seen in the non-operated contralateral superior rectus muscles. The ipsilateral inferior rectus showed reciprocal changes to the surgical superior rectus muscles.
Conclusions: The EOMs are extremely adaptive to changes induced by recession and tenotomy surgery, responding with modulations in fiber remodeling and myosin expression. These adaptive responses could be manipulated to improve surgical success rates.
Figures
Similar articles
-
The effect of resection on satellite cell activity in rabbit extraocular muscle.Invest Ophthalmol Vis Sci. 2006 Feb;47(2):605-13. doi: 10.1167/iovs.05-1069. Invest Ophthalmol Vis Sci. 2006. PMID: 16431957 Free PMC article.
-
Effects of elevated thyroid hormone on adult rabbit extraocular muscles.Invest Ophthalmol Vis Sci. 2010 Jan;51(1):183-91. doi: 10.1167/iovs.09-3681. Epub 2009 Jul 23. Invest Ophthalmol Vis Sci. 2010. PMID: 19628737 Free PMC article.
-
Changes in PAX7 Positive Satellite Cells in Extraocular Muscle After Strabismus Surgery.J Pediatr Ophthalmol Strabismus. 2025 May-Jun;62(3):190-195. doi: 10.3928/01913913-20241210-02. Epub 2025 Jan 21. J Pediatr Ophthalmol Strabismus. 2025. PMID: 39835589
-
Developmental, Physiological and Phylogenetic Perspectives on the Expression and Regulation of Myosin Heavy Chains in Craniofacial Muscles.Int J Mol Sci. 2024 Apr 21;25(8):4546. doi: 10.3390/ijms25084546. Int J Mol Sci. 2024. PMID: 38674131 Free PMC article. Review.
-
Minimal invasive vertical muscle transposition for the treatment of large angle exotropia due to congenital medial rectus hypoplasia: Case Report and Literature Review.Strabismus. 2020 Sep;28(3):158-162. doi: 10.1080/09273972.2020.1779320. Epub 2020 Jul 2. Strabismus. 2020. PMID: 32615839 Review.
Cited by
-
Effect of Fibroblast Growth Factor 2 on Extraocular Muscle Structure and Function.Invest Ophthalmol Vis Sci. 2021 Jul 1;62(9):34. doi: 10.1167/iovs.62.9.34. Invest Ophthalmol Vis Sci. 2021. PMID: 34293078 Free PMC article.
-
Prolongation of Relaxation Time in Extraocular Muscles With Brain Derived Neurotrophic Factor in Adult Rabbit.Invest Ophthalmol Vis Sci. 2016 Oct 1;57(13):5834-5842. doi: 10.1167/iovs.16-19679. Invest Ophthalmol Vis Sci. 2016. PMID: 27802489 Free PMC article.
-
Sustained release of bone morphogenetic protein-4 in adult rabbit extraocular muscle results in decreased force and muscle size: potential for strabismus treatment.Invest Ophthalmol Vis Sci. 2011 Jun 8;52(7):4021-9. doi: 10.1167/iovs.10-6878. Invest Ophthalmol Vis Sci. 2011. PMID: 21357389 Free PMC article.
-
Adaptability of the Immature Ocular Motor Control System: Unilateral IGF-1 Medial Rectus Treatment.Invest Ophthalmol Vis Sci. 2015 Jun;56(6):3484-96. doi: 10.1167/iovs.15-16761. Invest Ophthalmol Vis Sci. 2015. PMID: 26030103 Free PMC article.
-
Neural Plasticity Following Surgical Correction of Strabismus in Monkeys.Invest Ophthalmol Vis Sci. 2018 Oct 1;59(12):5011-5021. doi: 10.1167/iovs.18-25245. Invest Ophthalmol Vis Sci. 2018. PMID: 30326068 Free PMC article.
References
-
- Govindan M, Mohney BG, Diehl NN, Burke JP. Incidence and types of childhood exotropia: a population-based study. Ophthalmology. 2005;112:104–108 - PubMed
-
- Greenberg AR, Mohney BG, Diehl NN, Burke JP. Incidence and types of childhood esotropia: a population-based study. Ophthalmology. 2007;114:170–174 - PubMed
-
- Ganesh A, Pirouznia S, Ganguly SS, Fagerholm P, Lithander J. Consecutive exotropia after surgical treatment of childhood esotropia: a 40-year follow-up study. Acta Ophthalmol. Published online November 19, 2009 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
