

Hysterectomy-a comparison of approaches
- PMID: 20539807
- PMCID: PMC2883234
- DOI: 10.3238/arztebl.2010.0353
Hysterectomy-a comparison of approaches
Abstract
Background: The advantages and disadvantages of the various surgical techniques for hysterectomy are currently a topic of debate, with particular controversy over leaving the cervix in situ in the laparoscopic supracervical hysterectomy (LASH) procedure.
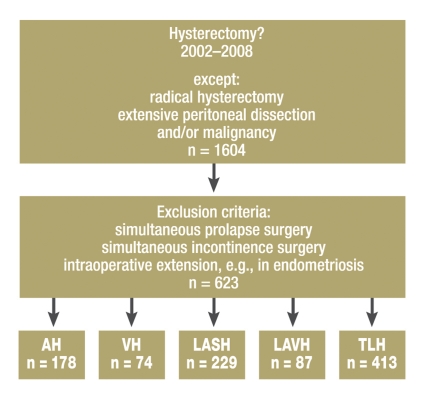
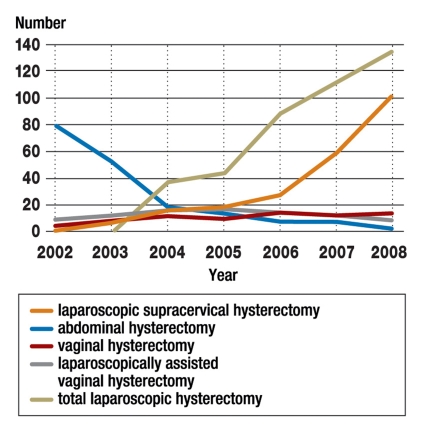
Methods: In a retrospective single-center study, medical history and clinical characteristics were compared in patients who had undergone hysterectomy for benign disease in the period 2002-2008 at the Department of Obstetrics and Gynecology, Erlangen University Hospital. Postoperative satisfaction and the frequency of secondary operations for prolapse or incontinence in women with surgery between 2002 and 2007 were surveyed by means of a questionnaire.
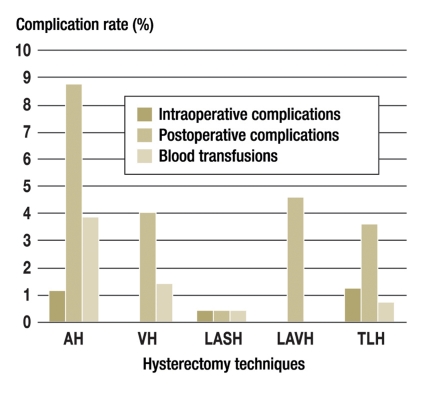
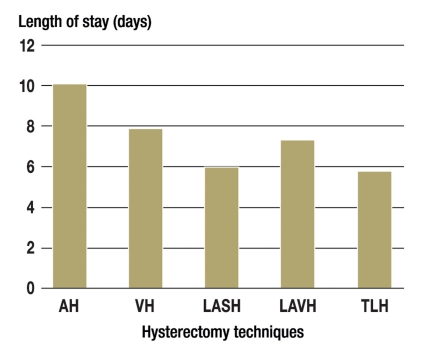
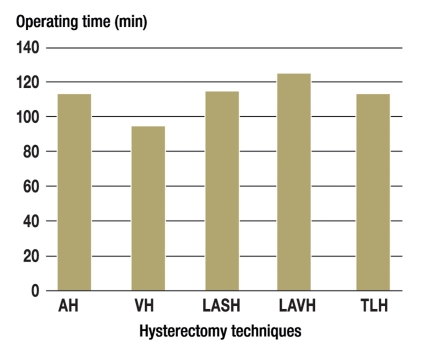
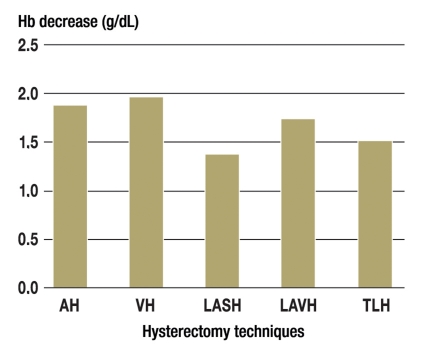
Results: The longest hospital stay was observed after abdominal hysterectomy (AH; 10 days), followed by vaginal hysterectomy (VH; 7.8 days) and laparoscopy-assisted vaginal hysterectomy (LAVH; 7.2 days). The shortest stays in hospital were seen after LASH (5.9 days) and total laparoscopic hysterectomy (TLH; 5.7 days). The shortest operating time was noted with VH (87 min) and the longest with LAVH (122 min). The lowest rates of blood loss were with LASH (1.38 g/dL) and TLH (1.51 g/dL). The highest rate of postoperative complications occurred after AH (8.9%). No differences were found in relation to postoperative satisfaction or surgery for prolapse or incontinence.
Conclusion: No postoperative benefits were found for leaving the cervix in situ when performing LASH. However, this was not a controlled randomized study.
Figures
Comment in
-
The marketing effect.Dtsch Arztebl Int. 2010 Nov;107(45):796; author reply 797-8. doi: 10.3238/arztebl.2010.0796b. Epub 2010 Nov 12. Dtsch Arztebl Int. 2010. PMID: 21124699 Free PMC article. No abstract available.
-
Patient welfare.Dtsch Arztebl Int. 2010 Nov;107(45):796; author reply 797-8. doi: 10.3238/arztebl.2010.0796a. Epub 2010 Nov 12. Dtsch Arztebl Int. 2010. PMID: 21124700 Free PMC article. No abstract available.
-
Six authors.Dtsch Arztebl Int. 2010 Nov;107(45):797; author reply 797-8. doi: 10.3238/arztebl.2010.0797a. Epub 2010 Nov 12. Dtsch Arztebl Int. 2010. PMID: 21124701 Free PMC article. No abstract available.
References
-
- Donnez O, Jadoul P, Squifet J, Donnez J. A series of 3190 laparoscopic hysterectomies for benign disease from 1990 to 2006: evaluation of complications compared with vaginal and abdominal procedures. BJOG. 2008 DOI: 10.1111/j.1471-0528.2008.01966.x. - PubMed
-
- Müller A, Thiel F, Binder H, et al. Myome - Teil 2. Geburtsh Frauenheilk. 2004;64:R245–R260.
-
- Müller A, Thiel F, Jud S, Beckmann MW, Renner S. Hysterektomie - was ist zeitgemäß? Geburtsh Frauenheilk. 2007;67:R101–R124.
-
- Altman D, Falconer C, Cnattingius S, Granath F. Pelvic organ prolapse surgery following hysterectomy on benign indications. Am J Obstet Gynecol. 2008;198:572, e1–e6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical