

Decubitus ulcers: pathophysiology and primary prevention
- PMID: 20539816
- PMCID: PMC2883282
- DOI: 10.3238/arztebl.2010.0371
Decubitus ulcers: pathophysiology and primary prevention
Abstract
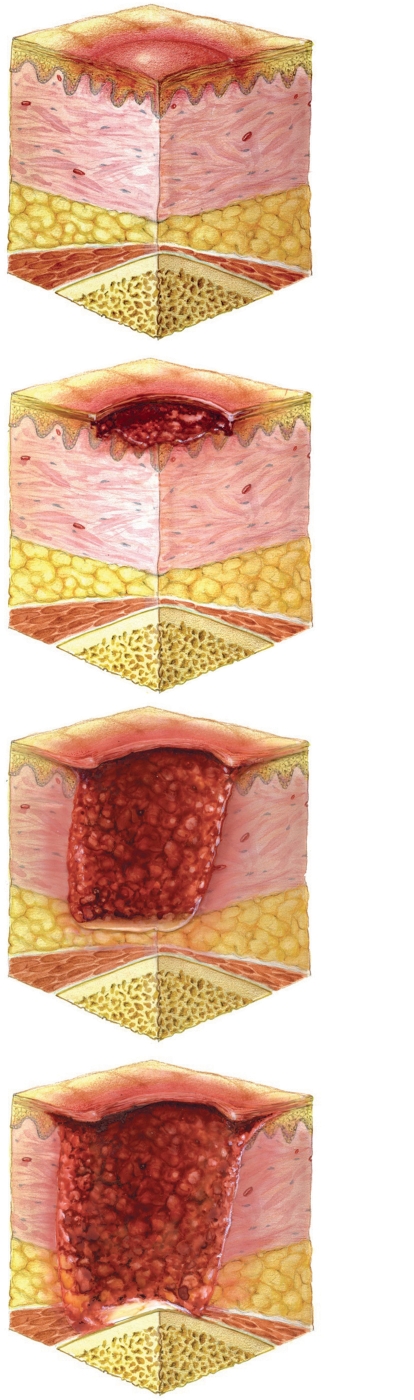
Background: Pressure sores are a serious complication of multimorbidity and lack of mobility. Decubitus ulcers have become rarer among bed-ridden patients because of the conscientious use of pressure-reducing measures and increased mobilization. Nonetheless, not all decubitus ulcers can be considered preventable or potentially curable, because poor circulation makes some patients more susceptible to them, and because cognitive impairment can make prophylactic measures difficult to apply.
Methods: A systematic literature search was performed in 2004 and 2005 in the setting of a health technology assessment, and a selective literature search was performed in 2009 for papers on the prevention of decubitus ulcers.
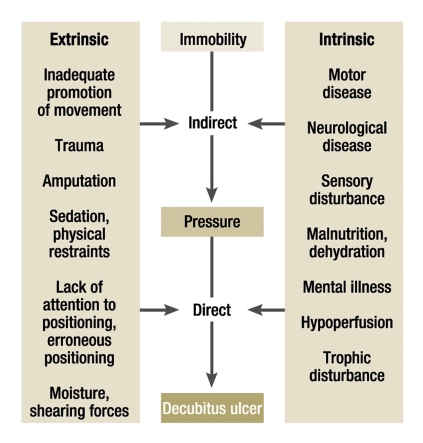
Results: Elderly, multimorbid patients with the immobility syndrome are at high risk for the development of decubitus ulcers, as are paraplegic patients. The most beneficial way to prevent decubitus ulcers, and to treat them once they are present, is to avoid excessive pressure by encouraging movement. At the same time, the risk factors that promote the development of decubitus ulcers should be minimized as far as possible.
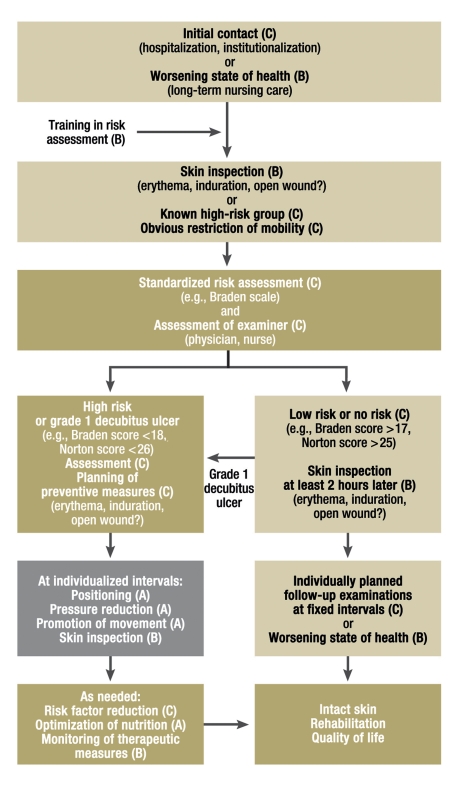
Conclusions: Malnutrition, poor circulation (hypoperfusion), and underlying diseases that impair mobility should be recognized if present and then treated, and accompanying manifestations, such as pain, should be treated symptomatically. Over the patient's further course, the feasibility, implementation, and efficacy of ulcer-preventing measures should be repeatedly re-assessed and documented, so that any necessary changes can be made. Risk factors for the development of decubitus ulcers should be assessed at the time of the physician's first contact with an immobile patient, or as soon as the patient's condition deteriorates; this is a prerequisite for timely prevention. Once the risks have been assessed, therapeutic measures should be undertaken on the basis of the patient's individual risk profile, with an emphasis on active encouragement of movement and passive relief of pressure through frequent changes of position.
Figures

Comment in
-
Identifying pain.Dtsch Arztebl Int. 2010 Oct;107(39):692; author reply 692. doi: 10.3238/arztebl.2010.0692a. Epub 2010 Oct 1. Dtsch Arztebl Int. 2010. PMID: 20963200 Free PMC article. No abstract available.
References
-
- Tillmann M. Zur Situation der Senioren in Hamburg und Umland - Ergebnisse einer rechtsmedizinischen Studie anlässlich der Krematoriumsleichenschau 2008 am Beispiel von Decubitalulcera. Medizinische Dissertation am Institut für Rechtsmedizin der Universität Hamburg, akzeptiert. 2010
-
- Krause T, Anders J, Heinemann A, et al. Ergebnisse einer Fall-Kontroll-Studie mit 200 Patienten und Befragung aller an der Pflege Beteiligten. Stuttgart: Kohlhammer; 2004. Ursachenzusammenhänge der Dekubitusentstehung.
-
- Eberhardt S, Heinemann A, Kulp W, et al. Health Technology Assessment Report: HTA-Bericht: Dekubitusprophylaxe und -therapie, DIMDI (eds) Köln, 2004. www.gripsdb.dimdi.de/de/hta/hta_berichte/hta128_bericht_de.pdf
-
- European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel. Prevention and treatment of pressure ulcers: clinical practice guideline. Washington DC: National Pressure Ulcer Advisory Panel; 2009. Zusammenfassungen als Download unter www.epuap.org/guidelines/Final_Quick_Prevention.pdf sowie www.epuap.org/guidelines/Final_Quick_Treatment.pdf.
-
- Black J, Baharestani M, Cuddigan J, et al. National Pressure Ulcer Advisory Panel’s updated pressure ulcer staging system. Dermatol Nurs. 2007;19:343–349. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical