

Heart rate control with adrenergic blockade: clinical outcomes in cardiovascular medicine
- PMID: 20539841
- PMCID: PMC2882891
- DOI: 10.2147/vhrm.s10358
Heart rate control with adrenergic blockade: clinical outcomes in cardiovascular medicine
Abstract
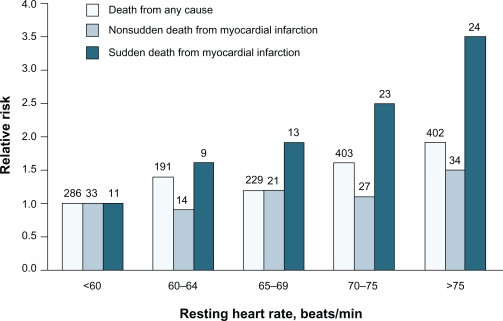
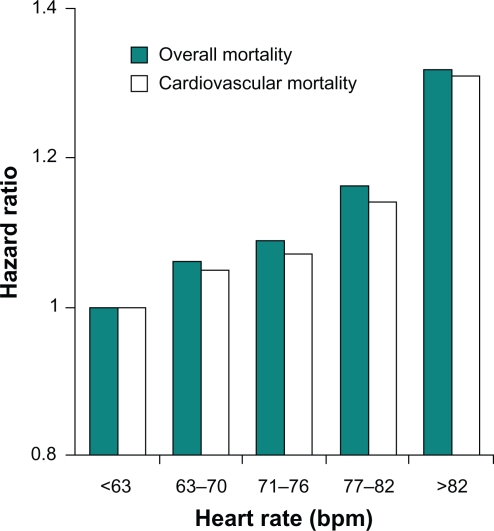
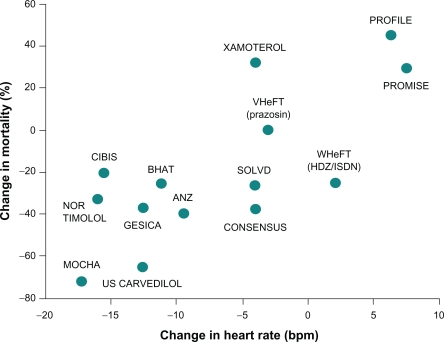
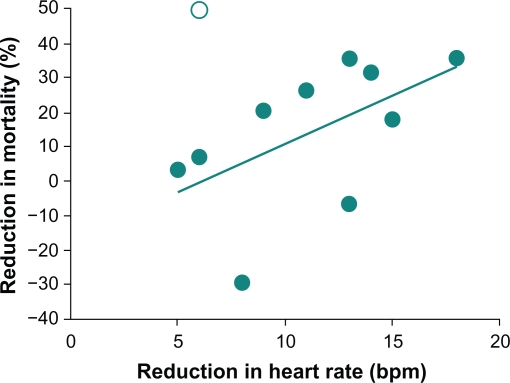
The sympathetic nervous system is involved in regulating various cardiovascular parameters including heart rate (HR) and HR variability. Aberrant sympathetic nervous system expression may result in elevated HR or decreased HR variability, and both are independent risk factors for development of cardiovascular disease, including heart failure, myocardial infarction, and hypertension. Epidemiologic studies have established that impaired HR control is linked to increased cardiovascular morbidity and mortality. One successful way of decreasing HR and cardiovascular mortality has been by utilizing beta-blockers, because their ability to alter cell signaling at the receptor level has been shown to mitigate the pathogenic effects of sympathetic nervous system hyperactivation. Numerous clinical studies have demonstrated that beta-blocker-mediated HR control improvements are associated with decreased mortality in postinfarct and heart failure patients. Although improved HR control benefits have yet to be established in hypertension, both traditional and vasodilating beta-blockers exert positive HR control effects in this patient population. However, differences exist between traditional and vasodilating beta-blockers; the latter reduce peripheral vascular resistance and exert neutral or positive effects on important metabolic parameters. Clinical evidence suggests that attainment of HR control is an important treatment objective for patients with cardiovascular conditions, and vasodilating beta-blocker efficacy may aid in accomplishing improved outcomes.
Keywords: adrenergic beta-antagonists; heart failure; hypertension; myocardial infarction.
Figures
References
-
- Lanza GA, Fox K, Crea F. Heart rate: A risk factor for cardiac diseases and outcomes? Pathophysiology of cardiac diseases and the potential role of heart rate slowing. Adv Cardiol. 2006;43:1–16. - PubMed
-
- Lurje L, Wennerblom B, Tygesen H, Karlsson T, Hjalmarson A. Heart rate variability after acute myocardial infarction in patients treated with atenolol and metoprolol. Int J Cardiol. 1997;60(2):157–164. - PubMed
-
- Lonn E, Grewal J. Drug therapies in the secondary prevention of cardiovascular diseases: Successes, shortcomings and future directions. Curr Vasc Pharmacol. 2006;4(3):253–268. - PubMed
-
- Poulter NR, Dobson JE, Sever PS, Dahlof B, Wedel H, Campbell NR. Baseline heart rate, antihypertensive treatment, and prevention of cardiovascular outcomes in ASCOT (Anglo – Scandinavian Cardiac Outcomes Trial) J Am Coll Cardiol. 2009;54(13):1154–1161. - PubMed
-
- Frishman WH. A historical perspective on the development of β-adrenergic blockers. J Clin Hypertens. 2007;9(4 Suppl 3):19–27.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
