

Pulse-pressure variation and hemodynamic response in patients with elevated pulmonary artery pressure: a clinical study
- PMID: 20540730
- PMCID: PMC2911757
- DOI: 10.1186/cc9060
Pulse-pressure variation and hemodynamic response in patients with elevated pulmonary artery pressure: a clinical study
Abstract
Introduction: Pulse-pressure variation (PPV) due to increased right ventricular afterload and dysfunction may misleadingly suggest volume responsiveness. We aimed to assess prediction of volume responsiveness with PPV in patients with increased pulmonary artery pressure.
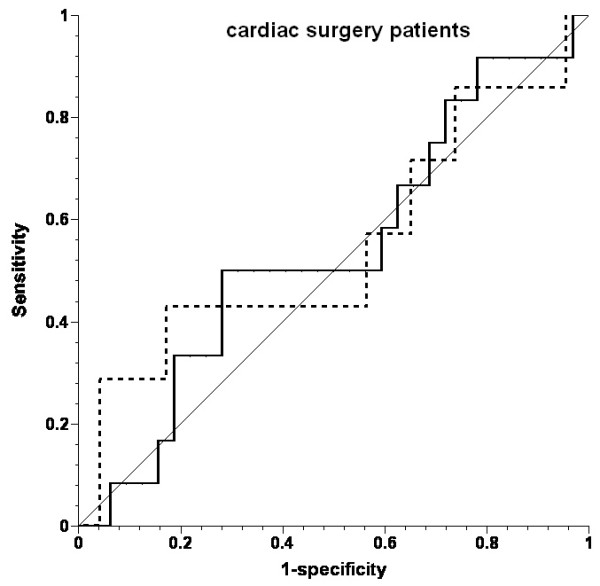
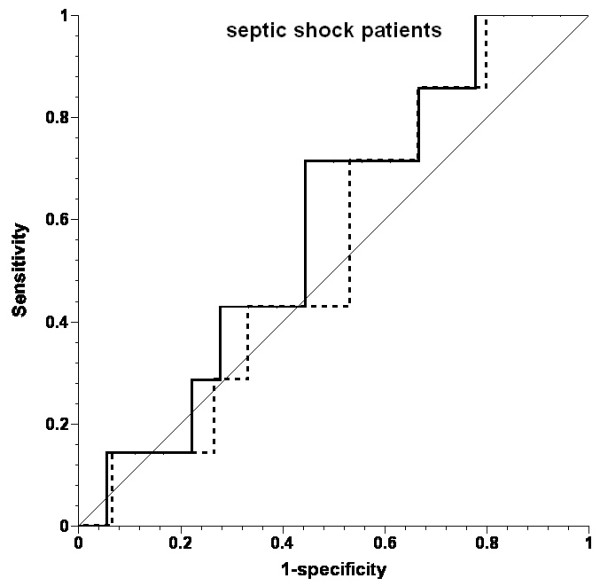
Methods: Fifteen cardiac surgery patients with a history of increased pulmonary artery pressure (mean pressure, 27 +/- 5 mm Hg (mean +/- SD) before fluid challenges) and seven septic shock patients (mean pulmonary artery pressure, 33 +/- 10 mm Hg) were challenged with 200 ml hydroxyethyl starch boli ordered on clinical indication. PPV, right ventricular ejection fraction (EF) and end-diastolic volume (EDV), stroke volume (SV), and intravascular pressures were measured before and after volume challenges.
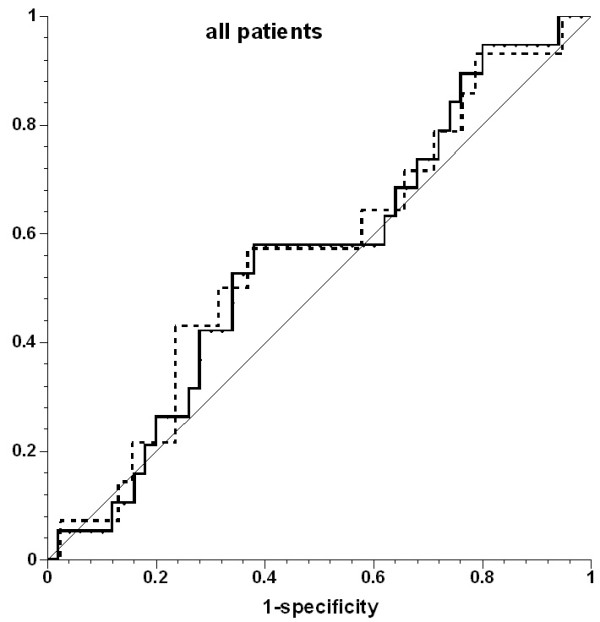
Results: Of 69 fluid challenges, 19 (28%) increased SV > 10%. PPV did not predict volume responsiveness (area under the receiver operating characteristic curve, 0.555; P = 0.485). PPV was >or=13% before 46 (67%) fluid challenges, and SV increased in 13 (28%). Right ventricular EF decreased in none of the fluid challenges, resulting in increased SV, and in 44% of those in which SV did not increase (P = 0.0003). EDV increased in 28% of fluid challenges, resulting in increased SV, and in 44% of those in which SV did not increase (P = 0.272).
Conclusions: Both early after cardiac surgery and in septic shock, patients with increased pulmonary artery pressure respond poorly to fluid administration. Under these conditions, PPV cannot be used to predict fluid responsiveness. The frequent reduction in right ventricular EF when SV did not increase suggests that right ventricular dysfunction contributed to the poor response to fluids.
Figures
Comment in
-
Further cautions for the use of ventilatory-induced changes in arterial pressures to predict volume responsiveness.Crit Care. 2010;14(5):197. doi: 10.1186/cc9223. Epub 2010 Sep 20. Crit Care. 2010. PMID: 20920155 Free PMC article. Review.
-
Using pulse pressure variation or stroke volume variation to diagnose right ventricular failure?Crit Care. 2010;14(6):451; author reply 451. doi: 10.1186/cc9303. Epub 2010 Nov 24. Crit Care. 2010. PMID: 21172070 Free PMC article. No abstract available.
Similar articles
-
Pulse pressure variation and volume responsiveness during acutely increased pulmonary artery pressure: an experimental study.Crit Care. 2010;14(3):R122. doi: 10.1186/cc9080. Epub 2010 Jun 24. Crit Care. 2010. PMID: 20576099 Free PMC article.
-
Pulse pressure variation is not a valid predictor of fluid responsiveness in patients with elevated left ventricular filling pressure.J Crit Care. 2014 Dec;29(6):987-91. doi: 10.1016/j.jcrc.2014.07.005. Epub 2014 Jul 10. J Crit Care. 2014. PMID: 25216949
-
Stroke Volume and Arterial Pressure Fluid Responsiveness in Patients With Elevated Stroke Volume Variation Undergoing Major Vascular Surgery: A Prospective Intervention Study.J Cardiothorac Vasc Anesth. 2023 Mar;37(3):407-414. doi: 10.1053/j.jvca.2022.11.028. Epub 2022 Nov 25. J Cardiothorac Vasc Anesth. 2023. PMID: 36529634
-
Fluid Challenge During Anesthesia: A Systematic Review and Meta-analysis.Anesth Analg. 2018 Dec;127(6):1353-1364. doi: 10.1213/ANE.0000000000003834. Anesth Analg. 2018. PMID: 30300177
-
Functional hemodynamic monitoring.Crit Care Clin. 2015 Jan;31(1):89-111. doi: 10.1016/j.ccc.2014.08.005. Crit Care Clin. 2015. PMID: 25435480 Free PMC article. Review.
Cited by
-
Cardiac filling volumes versus pressures for predicting fluid responsiveness after cardiovascular surgery: the role of systolic cardiac function.Crit Care. 2011;15(1):R73. doi: 10.1186/cc10062. Epub 2011 Feb 25. Crit Care. 2011. PMID: 21352541 Free PMC article. Clinical Trial.
-
Respiratory pulse pressure variation fails to predict fluid responsiveness in acute respiratory distress syndrome.Crit Care. 2011;15(2):R85. doi: 10.1186/cc10083. Epub 2011 Mar 7. Crit Care. 2011. PMID: 21385348 Free PMC article.
-
Pulmonary hypertension attenuates the dynamic preload indicators increase during experimental hypovolemia.BMC Anesthesiol. 2017 Mar 3;17(1):35. doi: 10.1186/s12871-017-0329-z. BMC Anesthesiol. 2017. PMID: 28253850 Free PMC article.
-
Co-existence of congestion and preload-dependence identified by pulse pressure respiratory variations: right ventricular afterload might be the key.Crit Care. 2025 Jul 1;29(1):262. doi: 10.1186/s13054-025-05440-5. Crit Care. 2025. PMID: 40598584 Free PMC article. No abstract available.
-
Impact of norepinephrine on the relationship between pleth variability index and pulse pressure variations in ICU adult patients.Crit Care. 2011 Jul 12;15(4):R168. doi: 10.1186/cc10310. Crit Care. 2011. PMID: 21749695 Free PMC article.
