

Percutaneous ablation of adrenal tumors
- PMID: 20540918
- PMCID: PMC2886030
- DOI: 10.1053/j.tvir.2010.02.004
Percutaneous ablation of adrenal tumors
Abstract
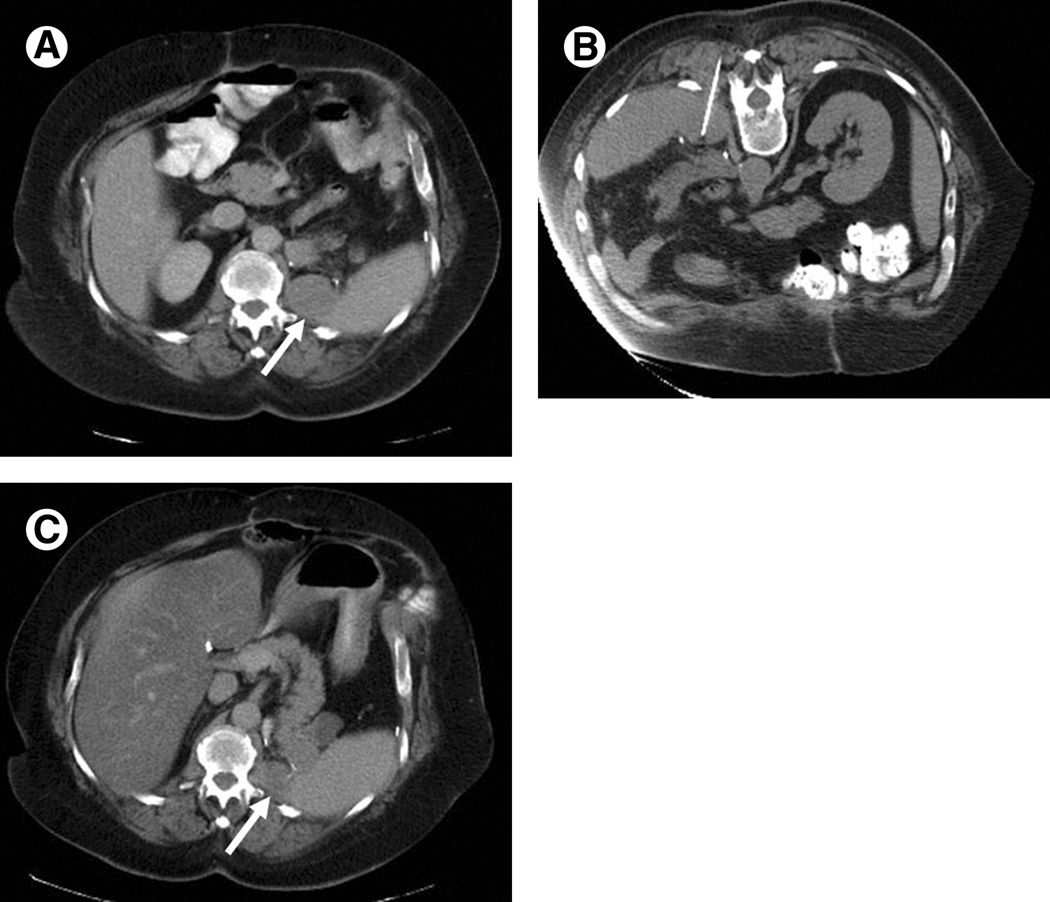
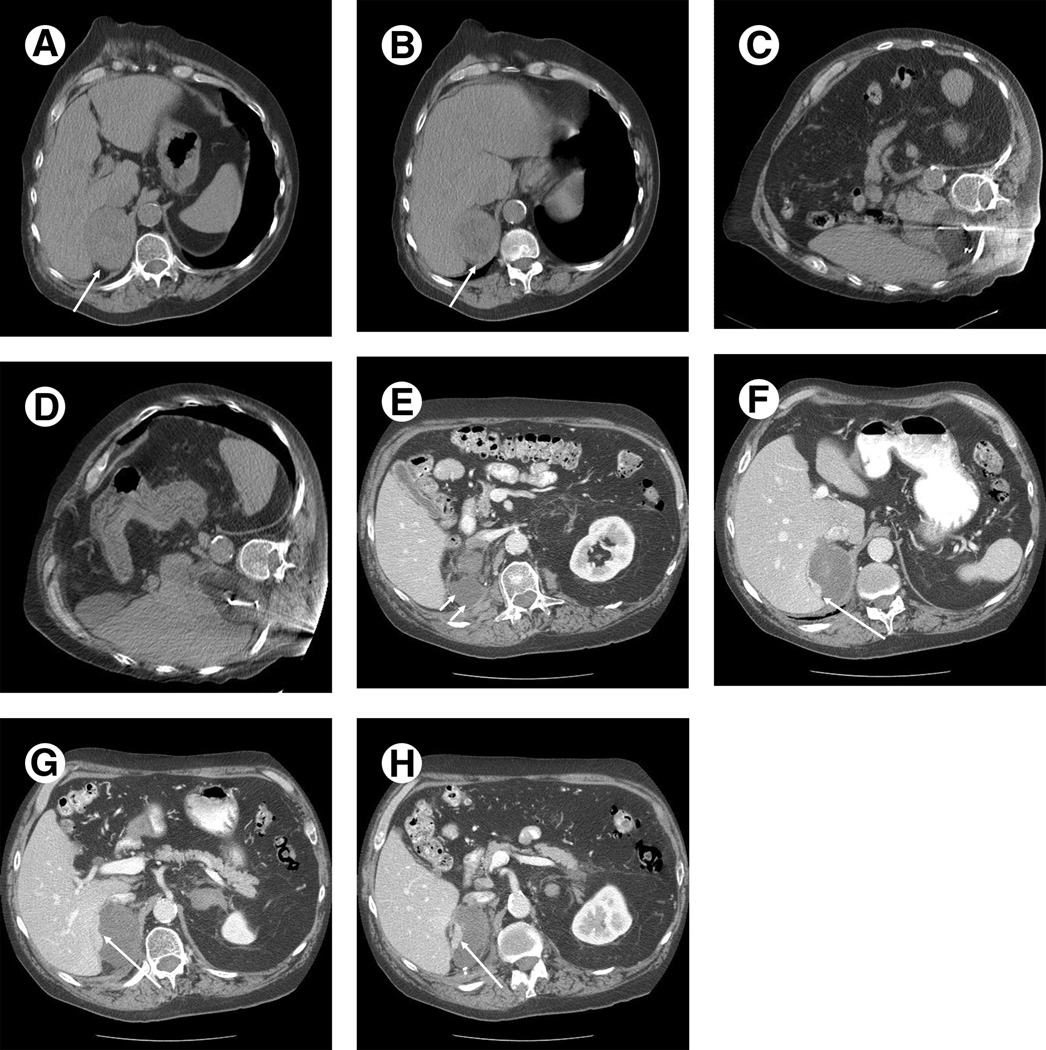
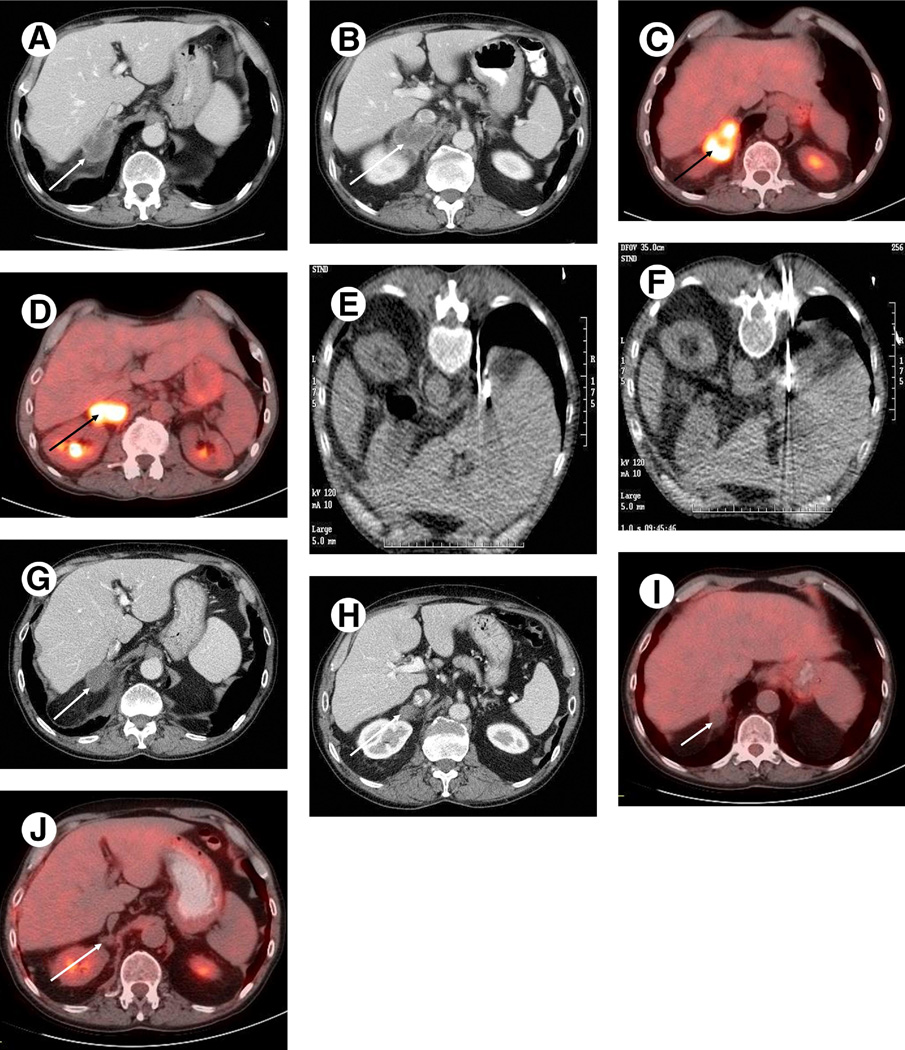
Adrenal tumors comprise a broad spectrum of benign and malignant neoplasms and include functional adrenal adenomas, pheochromocytomas, primary adrenocortical carcinoma, and adrenal metastases. Percutaneous ablative approaches that have been described and used in the treatment of adrenal tumors include percutaneous radiofrequency ablation, cryoablation, microwave ablation, and chemical ablation. Local tumor ablation in the adrenal gland presents unique challenges, secondary to the adrenal gland's unique anatomic and physiological features. The results of clinical series employing percutaneous ablative techniques in the treatment of adrenal tumors are reviewed in this article. Clinical and technical considerations unique to ablation in the adrenal gland are presented, including approaches commonly used in our practices, and risks and potential complications are discussed.
Published by Elsevier Inc.
Figures
References
-
- Beland M, Mayo-Smith W. Ablation of adrenal neoplasms. Abdom Imaging. 2009;34:588–592. - PubMed
-
- Carrafiello G, Lagana D, Recaldini C, et al. Imaging-guided percutaneous radiofrequency ablation of adrenal metastases: preliminary results at a single institution with a single device. Cardiovasc Intervent Radiol. 2008;31:762–767. - PubMed
-
- Abrams H, Spiro R, Goldstein N. Metastasis in carcinoma: analysis of 1000 autopsied cases. Cancer. 1950;3:74–85. - PubMed
-
- Bullock W, Hirst AJ. Metastatic carcinoma of the adrenal. Am J Med Sci. 1953;226:521–524. - PubMed
-
- Cedermark B, Blumenson L, Pickren J, et al. The significant of metastases to the adrenal glands in adenocarcinoma of the colon and rectum. Surg Gynecol Obstet. 1977;144:537–546. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
