

An integrative model of respiratory and cardiovascular control in sleep-disordered breathing
- PMID: 20542148
- PMCID: PMC2965826
- DOI: 10.1016/j.resp.2010.06.001
An integrative model of respiratory and cardiovascular control in sleep-disordered breathing
Abstract
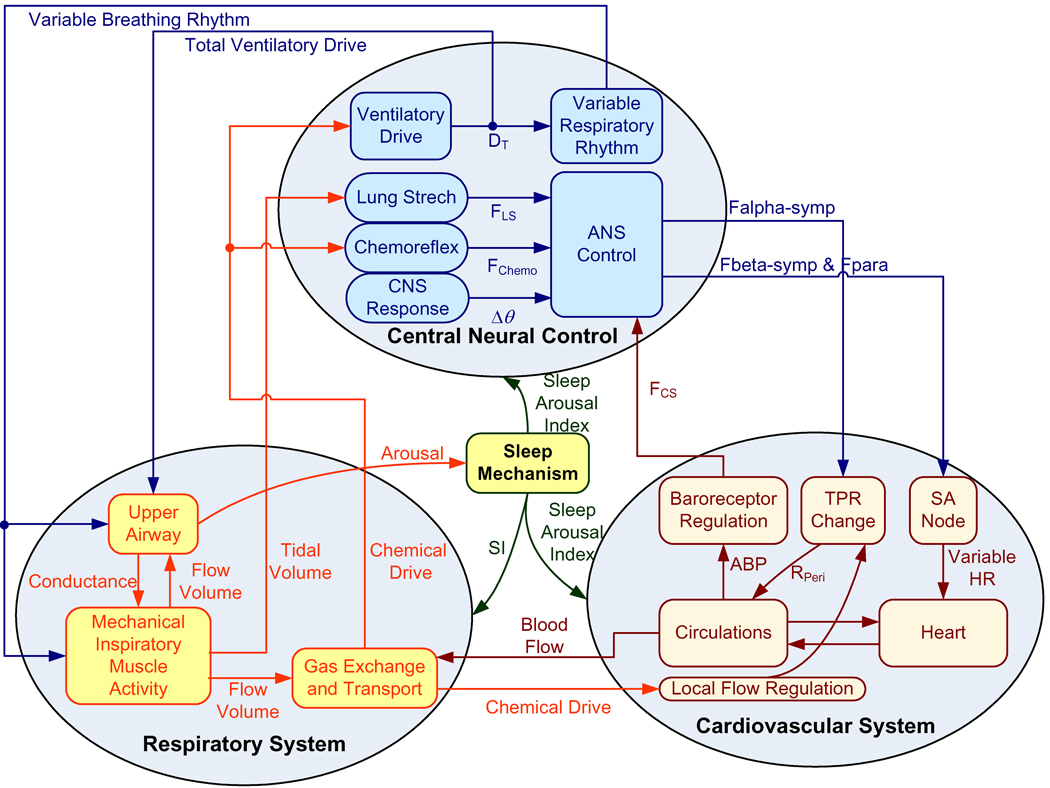
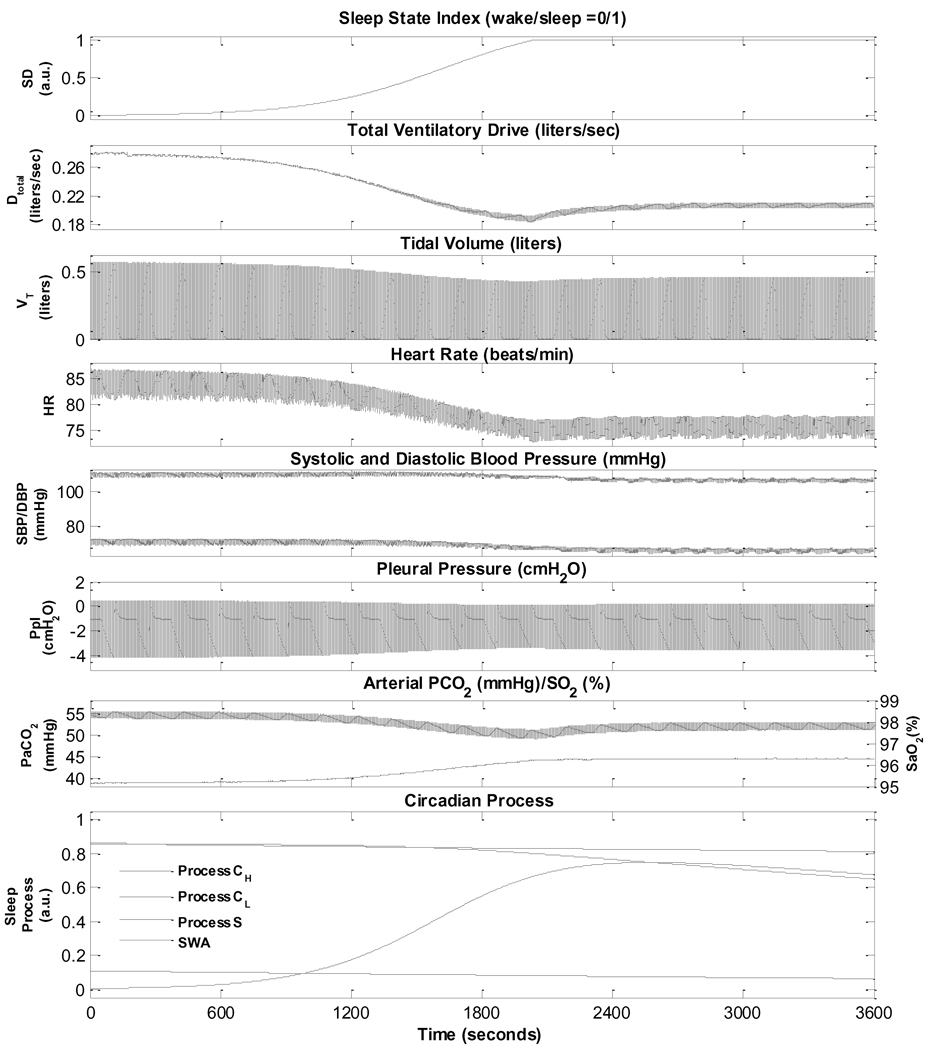
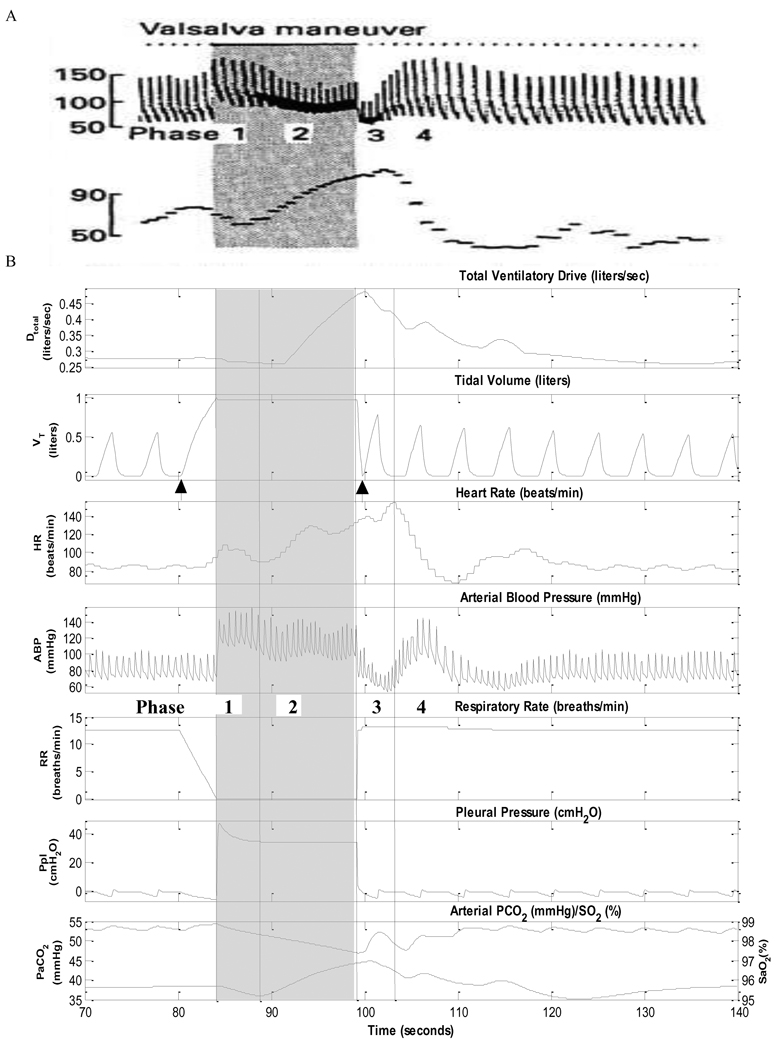
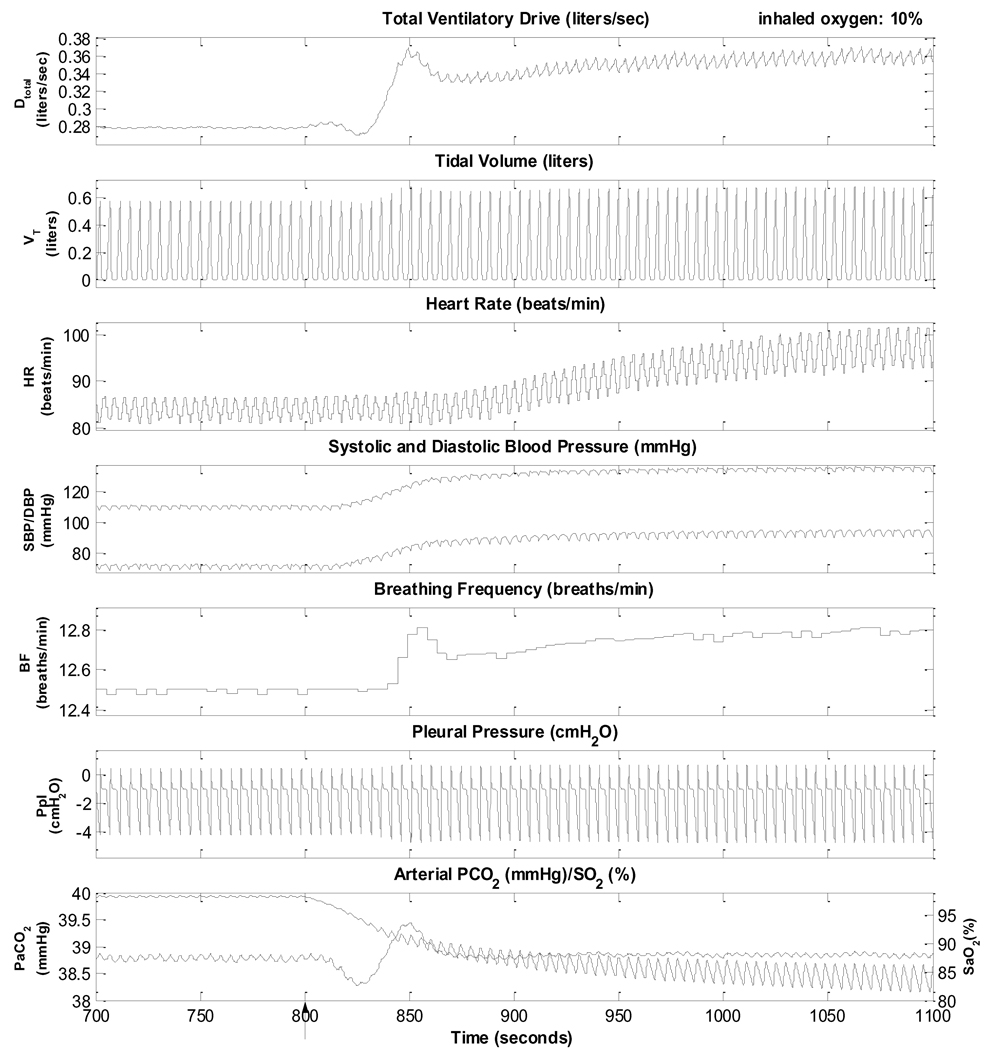
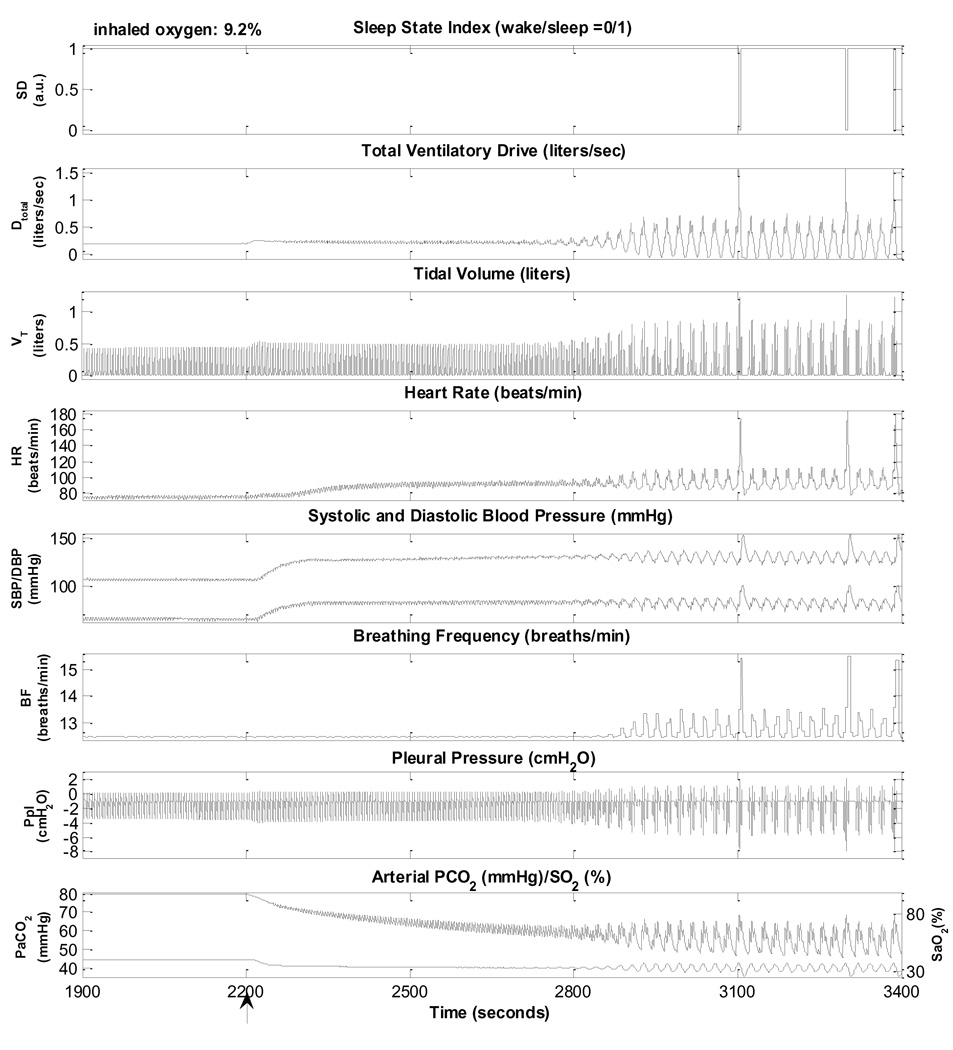
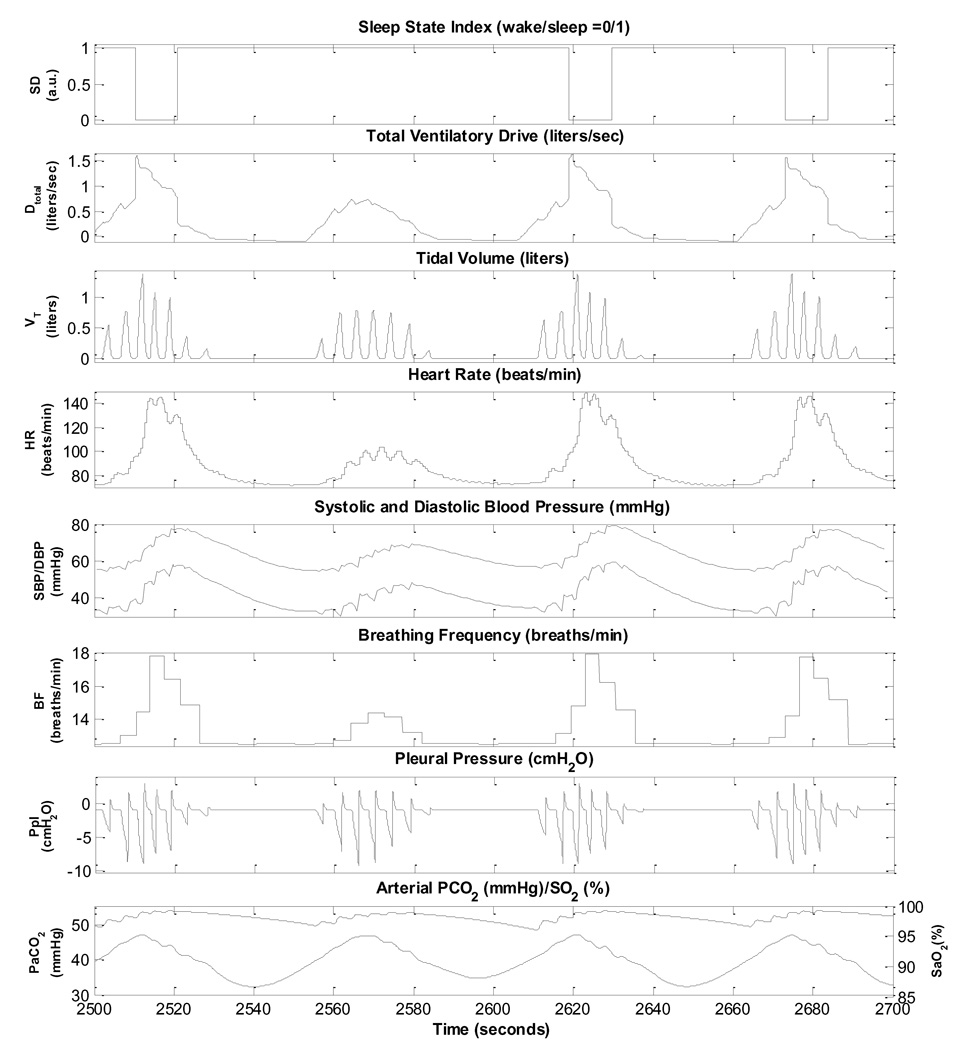
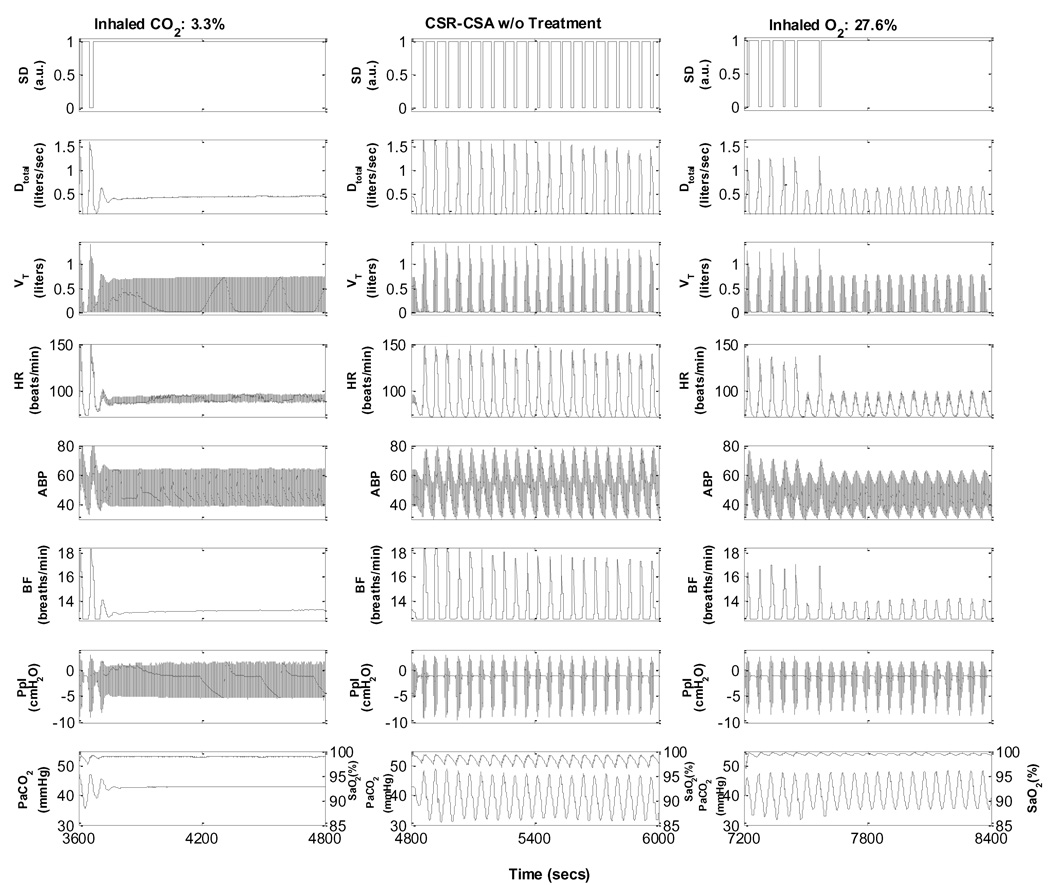
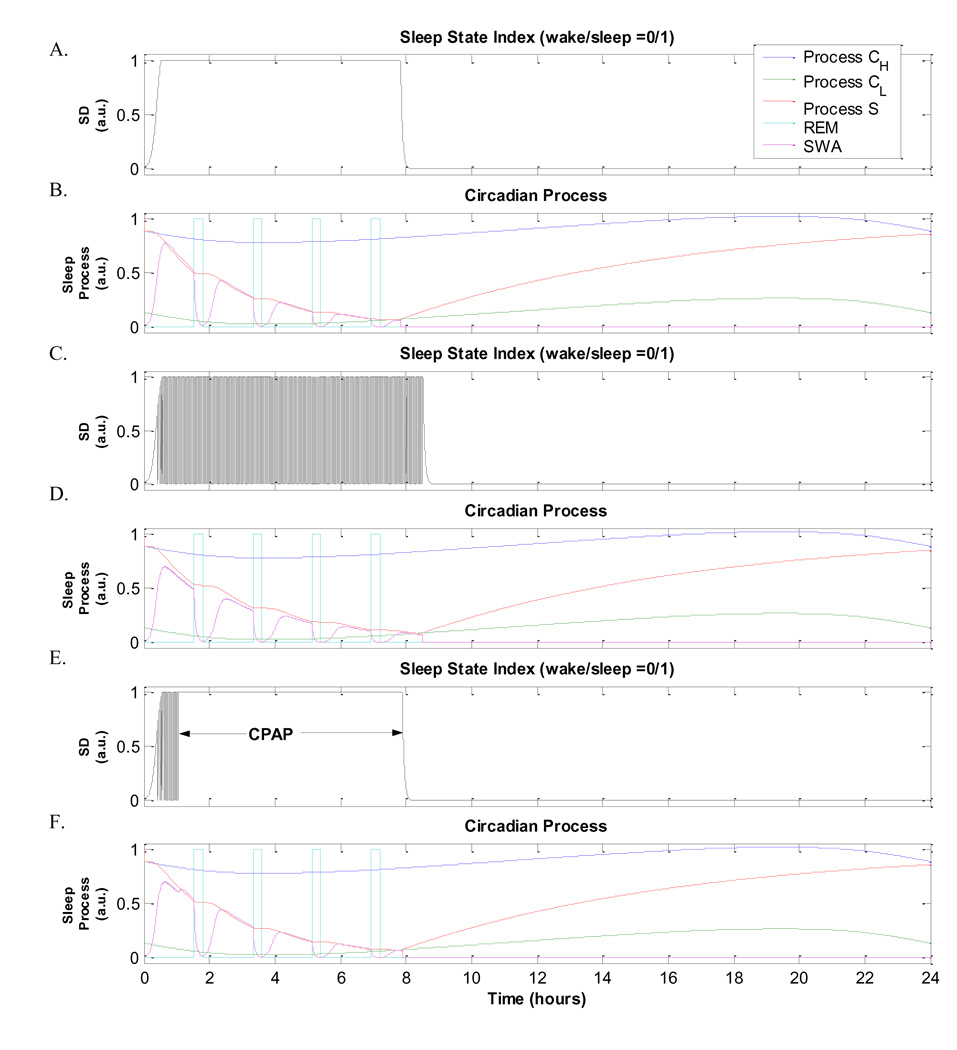
While many physiological control models exist in the literature, none thus far has focused on characterizing the interactions among the respiratory, cardiovascular and sleep-wake regulation systems that occur in sleep-disordered breathing. The model introduced in this study integrates the autonomic control of the cardiovascular system, chemoreflex and state-related control of respiration, including respiratory and upper airway mechanics, along with a model of circadian and sleep-wake regulation. The integrative model provides realistic predictions of the physiological responses under a variety of conditions including: the sleep-wake cycle, hypoxia-induced periodic breathing, Cheyne-Stokes respiration in chronic heart failure, and obstructive sleep apnoea (OSA). It can be used to investigate the effects of a variety of interventions, such as isocapnic and hypercapnic and/or hypoxic gas administration, the Valsalva and Mueller maneuvers, and the application of continuous positive airway pressure on OSA subjects. By being able to delineate the influences of the various interacting physiological mechanisms, the model is useful in providing a more lucid understanding of the complex dynamics that characterize state-cardiorespiratory control in the different forms of sleep-disordered breathing.
Copyright © 2010 Elsevier B.V. All rights reserved.
Figures
References
-
- Achermann P, Borbely AA. Mathematical models of sleep regulation. Frontiers in Biosci. 2003;8:s683–s693. - PubMed
-
- Andreas S, Hagenah G, Moller C, Werner GS, Kreuzer H. Cheyne-Stokes respiration and prognosis in congestive heart failure. Am J Cardiol. 1996;78:1260–1264. - PubMed
-
- Bai J, Lu H, Zhang J, Zhou X. Simulation study of the interaction between respiration and the cardiovascular system. Methods Inf Med. 1997;36:261–263. - PubMed
-
- Bannister R. Defective baroreflex function in autonomic failure. In: Sleight P, editor. Arterial baroreceptors and hypertension. Oxford, UK: Oxford University Press; 1980. pp. 117–122.
-
- Baust W, Bohnert B. The regulation of heart rate during sleep. Exp Brain Res. 1969;7:169–180. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
