

Exercise hemodynamics enhance diagnosis of early heart failure with preserved ejection fraction
- PMID: 20543134
- PMCID: PMC3048586
- DOI: 10.1161/CIRCHEARTFAILURE.109.930701
Exercise hemodynamics enhance diagnosis of early heart failure with preserved ejection fraction
Abstract
Background: When advanced, heart failure with preserved ejection fraction (HFpEF) is readily apparent. However, diagnosis of earlier disease may be challenging because exertional dyspnea is not specific for heart failure, and biomarkers and hemodynamic indicators of volume overload may be absent at rest.
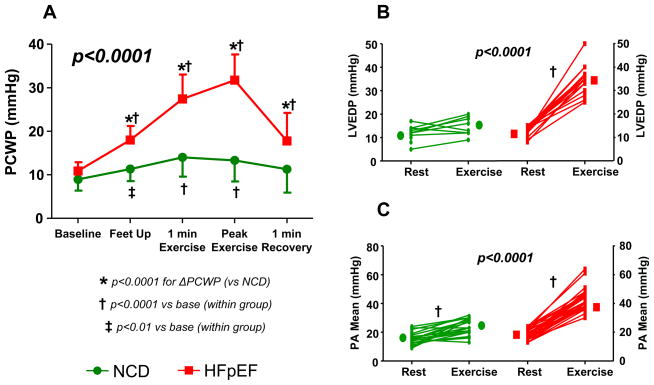
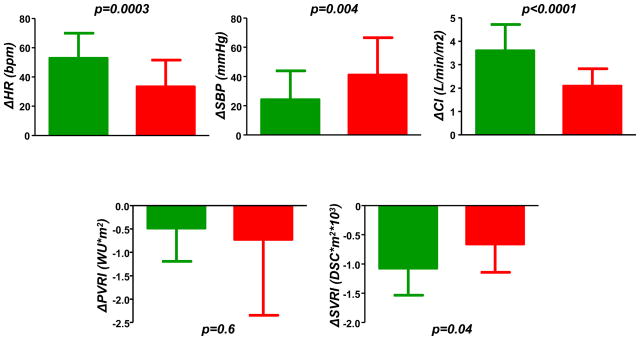
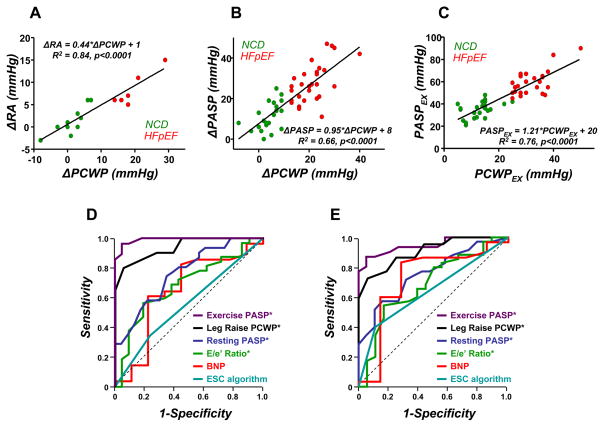
Methods and results: Patients with exertional dyspnea and ejection fraction >50% were referred for hemodynamic catheterization. Those with no significant coronary disease, normal brain natriuretic peptide assay, and normal resting hemodynamics (mean pulmonary artery pressure <25 mm Hg and pulmonary capillary wedge pressure [PCWP] <15 mm Hg) (n=55) underwent exercise study. The exercise PCWP was used to classify patients as having HFpEF (PCWP ≥25 mm Hg) (n=32) or noncardiac dyspnea (PCWP <25 mm Hg) (n=23). At rest, patients with HFpEF had higher resting pulmonary artery pressure and PCWP, although all values fell within normal limits. Exercise-induced elevation in PCWP in HFpEF was confirmed by greater increases in left ventricular end-diastolic pressure and was associated with blunted increases in heart rate, systemic vasodilation, and cardiac output. Exercise-induced pulmonary hypertension was present in 88% of patients with HFpEF and was related principally to elevated PCWP, as pulmonary vascular resistances dropped similarly in both groups. Exercise PCWP and pulmonary artery systolic pressure were highly correlated. An exercise pulmonary artery systolic pressure ≥45 mm Hg identified HFpEF with 96% sensitivity and 95% specificity.
Conclusions: Euvolemic patients with exertional dyspnea, normal brain natriuretic peptide, and normal cardiac filling pressures at rest may have markedly abnormal hemodynamic responses during exercise, suggesting that chronic symptoms are related to heart failure. Earlier and more accurate diagnosis using exercise hemodynamics may allow better targeting of interventions to treat and prevent HFpEF progression.
Figures
References
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–259. - PubMed
-
- Bhatia RS, Tu JV, Lee DS, Austin PC, Fang J, Haouzi A, Gong Y, Liu PP. Outcome of heart failure with preserved ejection fraction in a population-based study. N Engl J Med. 2006;355:260–269. - PubMed
-
- Bursi F, Weston SA, Redfield MM, Jacobsen SJ, Pakhomov S, Nkomo VT, Meverden RA, Roger VL. Systolic and diastolic heart failure in the community. Jama. 2006;296:2209–2216. - PubMed
-
- Klapholz M, Maurer M, Lowe AM, Messineo F, Meisner JS, Mitchell J, Kalman J, Phillips RA, Steingart R, Brown EJ, Jr, Berkowitz R, Moskowitz R, Soni A, Mancini D, Bijou R, Sehhat K, Varshneya N, Kukin M, Katz SD, Sleeper LA, Le Jemtel TH. Hospitalization for heart failure in the presence of a normal left ventricular ejection fraction: results of the New York Heart Failure Registry. J Am Coll Cardiol. 2004;43:1432–1438. - PubMed
-
- Davie AP, Francis CM, Caruana L, Sutherland GR, McMurray JJ. Assessing diagnosis in heart failure: which features are any use? Qjm. 1997;90:335–339. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
