

Organ reengineering through development of a transplantable recellularized liver graft using decellularized liver matrix
- PMID: 20543851
- PMCID: PMC2930603
- DOI: 10.1038/nm.2170
Organ reengineering through development of a transplantable recellularized liver graft using decellularized liver matrix
Abstract
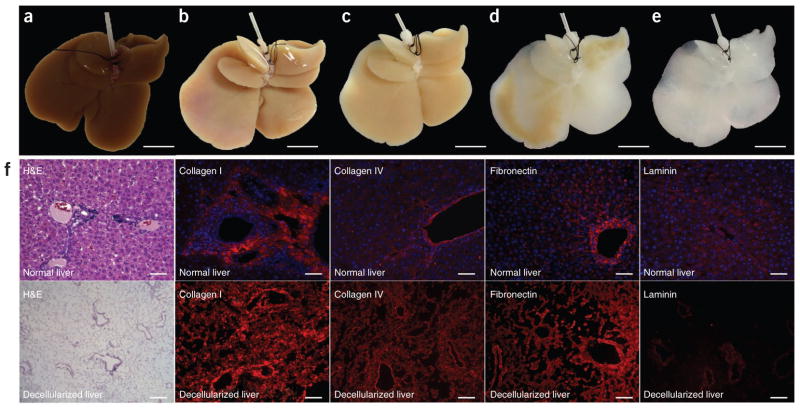
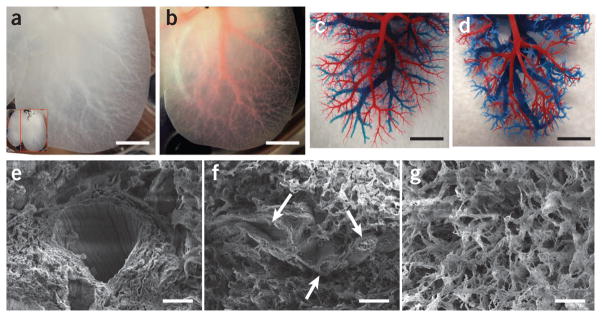
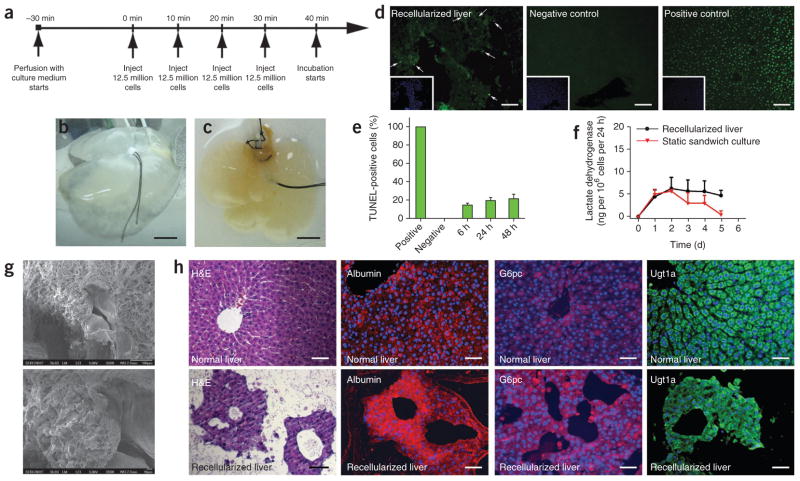
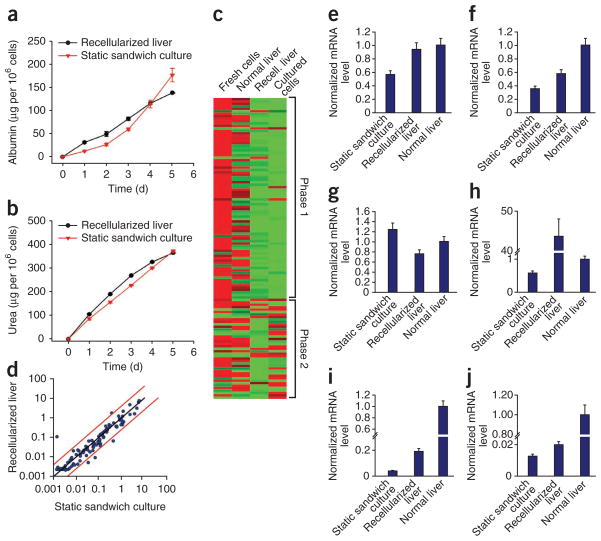
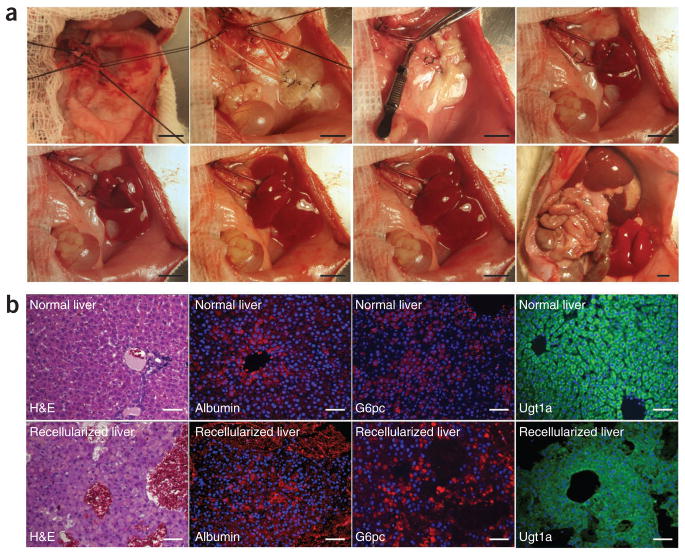
Orthotopic liver transplantation is the only available treatment for severe liver failure, but it is currently limited by organ shortage. One technical challenge that has thus far limited the development of a tissue-engineered liver graft is oxygen and nutrient transport. Here we demonstrate a novel approach to generate transplantable liver grafts using decellularized liver matrix. The decellularization process preserves the structural and functional characteristics of the native microvascular network, allowing efficient recellularization of the liver matrix with adult hepatocytes and subsequent perfusion for in vitro culture. The recellularized graft supports liver-specific function including albumin secretion, urea synthesis and cytochrome P450 expression at comparable levels to normal liver in vitro. The recellularized liver grafts can be transplanted into rats, supporting hepatocyte survival and function with minimal ischemic damage. These results provide a proof of principle for the generation of a transplantable liver graft as a potential treatment for liver disease.
Conflict of interest statement
The authors declare no competing financial interests.
Figures
Comment in
-
Lab-grown organs seen as remedy for long donor waitlists.Nat Med. 2010 Aug;16(8):834. doi: 10.1038/nm0810-834b. Nat Med. 2010. PMID: 20689531 No abstract available.
-
Liver: Proof of principle for the generation of a transplantable recellularized liver graft.Nat Rev Gastroenterol Hepatol. 2010 Aug;7(8):415. doi: 10.1038/nrgastro.2010.106. Nat Rev Gastroenterol Hepatol. 2010. PMID: 20712069 No abstract available.
-
The recellularized liver matrix: a novel way of transplantation?Hepatology. 2010 Oct;52(4):1509-11. doi: 10.1002/hep.23956. Hepatology. 2010. PMID: 20879031 No abstract available.
-
A reengineered liver for transplantation.J Hepatol. 2011 Feb;54(2):386-7. doi: 10.1016/j.jhep.2010.07.053. Epub 2010 Nov 10. J Hepatol. 2011. PMID: 21112113 No abstract available.
References
-
- Heron M, et al. National Vital Statistics Report. Vol. 57. Centers for Disease Control and Prevention; Hyattsville, Maryland: 2009. Deaths: Final Data for 2006. - PubMed
-
- Punch JD, Hayes DH, LaPorte FB, McBride V, Seely MS. Organ donation and utilization in the United States, 1996–2005. Am J Transplant. 2007;7:1327–1338. - PubMed
-
- Fox IJ, Roy-Chowdhury J. Hepatocyte transplantation. J Hepatol. 2004;40:878–886. - PubMed
-
- Strom SC, et al. Hepatocyte transplantation as a bridge to orthotopic liver transplantation in terminal liver failure. Transplantation. 1997;63:559–569. - PubMed
-
- Horslen SP, et al. Isolated hepatocyte transplantation in an infant with a severe urea cycle disorder. Pediatrics. 2003;111:1262–1267. - PubMed
Publication types
MeSH terms
Grants and funding
- K99 DK088962/DK/NIDDK NIH HHS/United States
- K99 DK080942/DK/NIDDK NIH HHS/United States
- R00 DK088962/DK/NIDDK NIH HHS/United States
- R01 DK059766/DK/NIDDK NIH HHS/United States
- K99 DK083556/DK/NIDDK NIH HHS/United States
- K99DK083556/DK/NIDDK NIH HHS/United States
- R00 DK083556/DK/NIDDK NIH HHS/United States
- R01 DK084053/DK/NIDDK NIH HHS/United States
- R00 DK080942/DK/NIDDK NIH HHS/United States
- R01DK59766/DK/NIDDK NIH HHS/United States
- R01DK084053/DK/NIDDK NIH HHS/United States
- K99/R00 DK080942/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
