

The radiographic approach to child abuse
- PMID: 20544318
- PMCID: PMC3032862
- DOI: 10.1007/s11999-010-1414-5
The radiographic approach to child abuse
Abstract
Background: Osseous injuries are a major facet of child abuse and in most patients radiographic imaging plays a major role in diagnosis. While some injuries are typically produced as a result of excessive and inappropriate force other injuries are nonspecific in terms of their causation, but become suspicious when the history provided by the caretakers is inconsistent with the type of injury produced.
Questions/purposes: I detail the radiographic imaging of the more characteristic of the highly specific injuries, discuss the major issues that relate to some moderate- or low-specificity injuries, and describe several diseases that mimic abuse.
Methods: A review of the current and recent literature focused on the radiographic imaging of child abuse was performed by searching the National Library of Medicine database at pubmed.gov. Keywords used included: radiology, fracture, child abuse, and/or nonaccidental trauma.
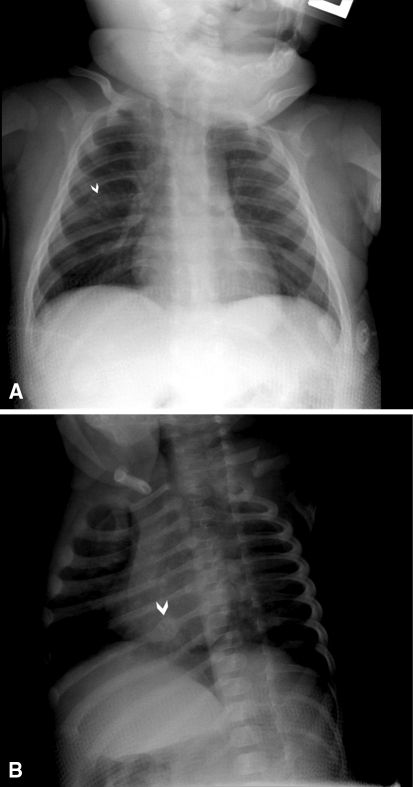
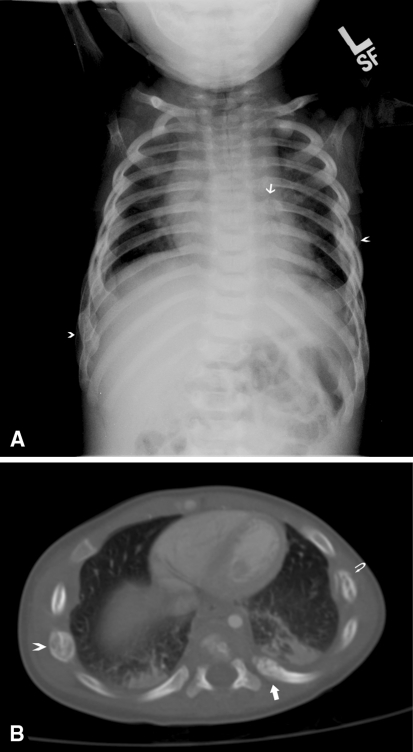
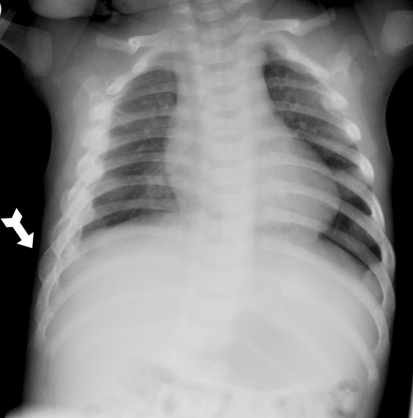
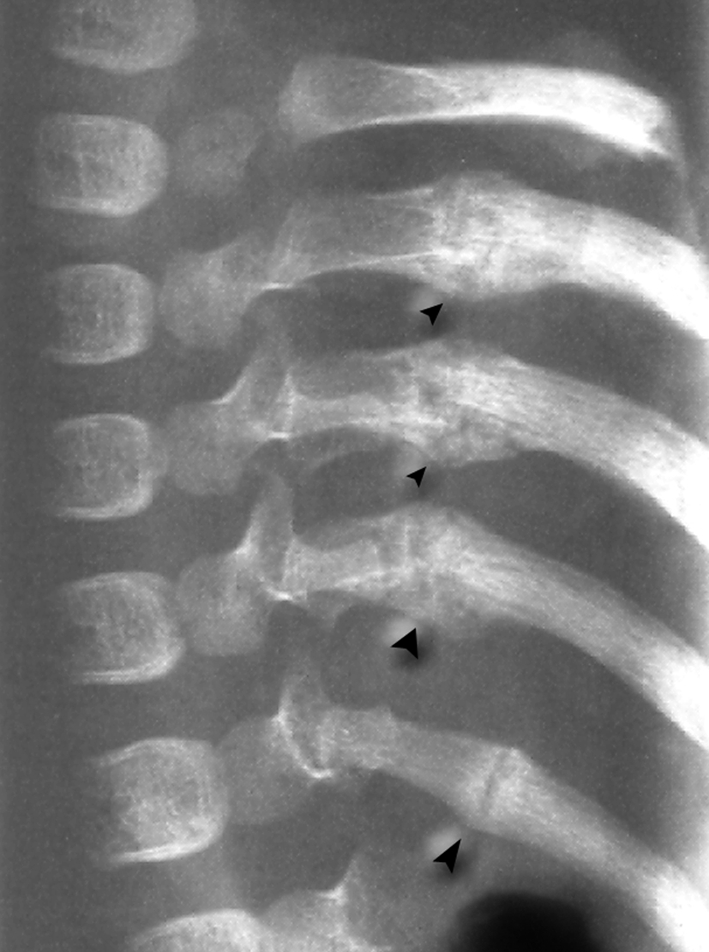
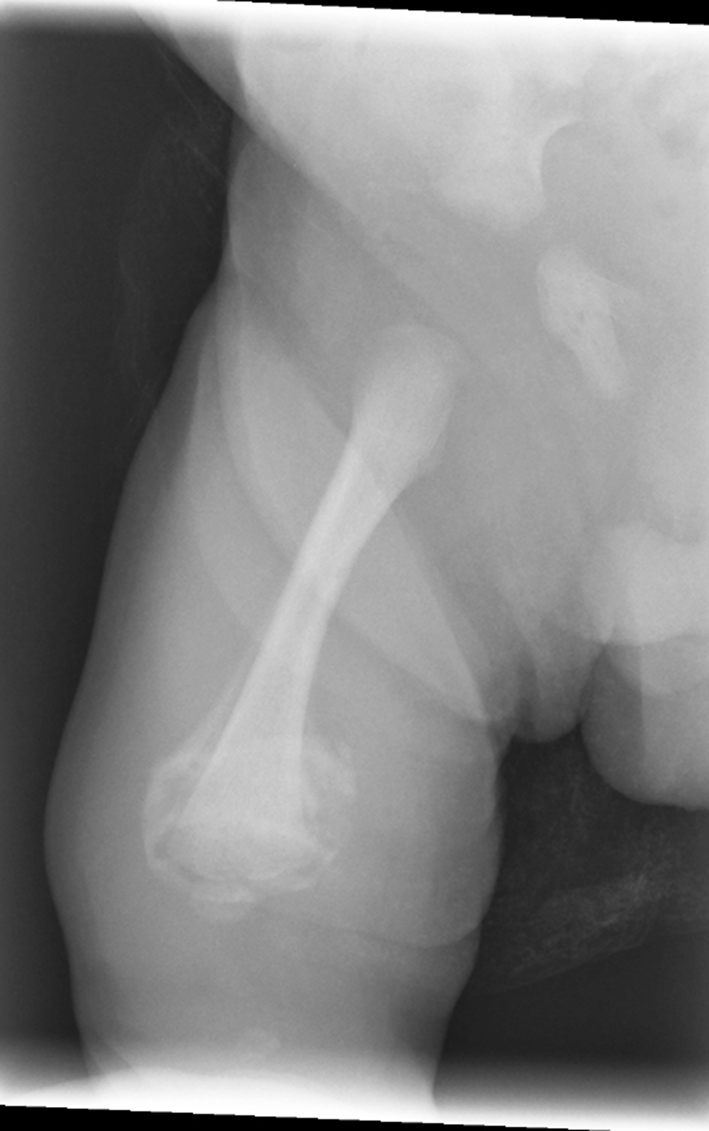
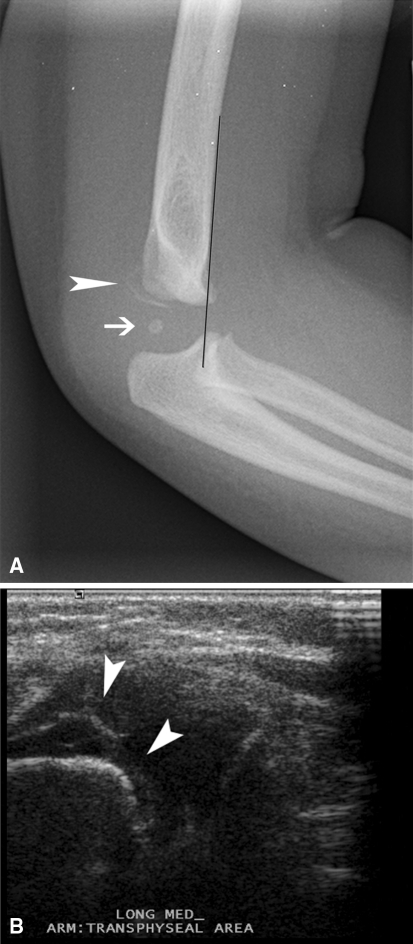
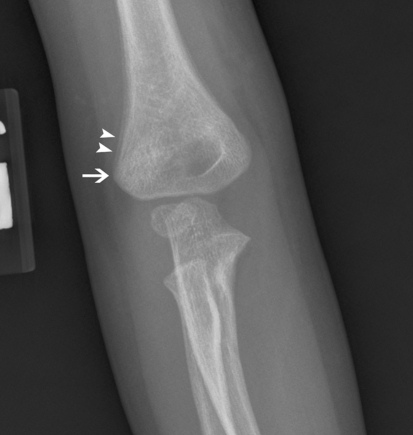
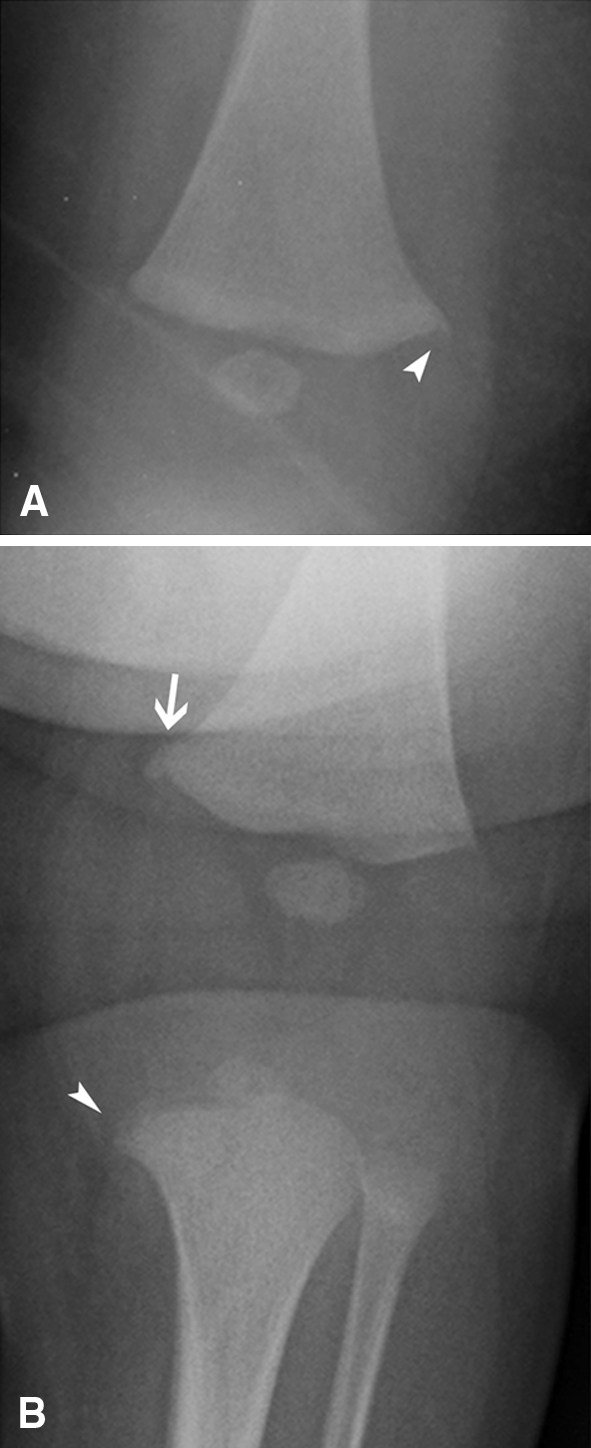
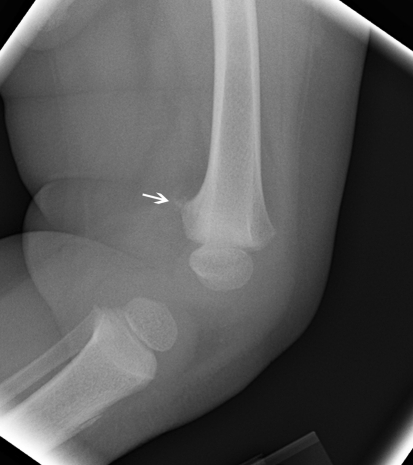
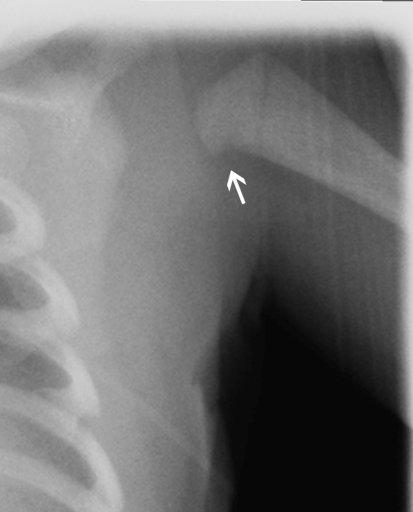
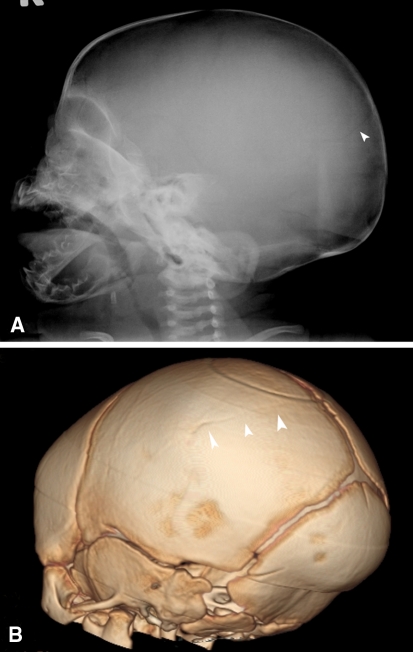
Results: Injuries that are highly specific for the diagnosis of abuse include metaphyseal corner fractures, posteromedial rib fractures, and sternal, scapular, and spinous process fractures. Lesions of moderate specificity include, among other injuries, multiple fractures of various ages and epiphyseal separations. Long-bone fractures and clavicular fractures, while common, are of low specificity. In addition to the appropriate accurate diagnosis of these injuries, several diseases and syndromes may mimic abuse due to the similarity in the radiographic picture.
Conclusions: Stratification of fractures sustained in child abuse according to specificity and an understanding of the several diseases that mimic abuse are helpful in the accurate diagnosis of child abuse.
Level of evidence: Level V, diagnostic study. See Guidelines for Authors for a complete description of levels of evidence.
Figures


References
-
- Adams PC, Strand RD, Bresnan MJ, Lucky AW. Kinky hair syndrome: serial study of radiological findings with emphasis on the similarity to the battered child syndrome. Radiology. 1974;112:401–407. - PubMed
-
- American College of Radiology. ACR practice guideline for skeletal surveys in children. Available at: http://www.acr.org/SecondaryMainMenuCategories/quality_safety/guidelines.... Accessed September 11, 2009.
-
- Baldridge D, Schwarze U, Morello R, Lennington J, Bertin TK, Pace JM, Pepin MG, Weis M, Eyre DR, Walsh J, Lambert D, Green A, Robinson H, Michelson M, Houge G, Lindman C, Martin J, Ward J, Lemyre E, Mitchell JJ, Krakow D, Rimoin DL, Cohn DH, Byers PH, Lee B. CRTAP and LEPRE1 mutations in recessive osteogenesis imperfecta. Hum Mutat. 2008;29:1435–1442. doi: 10.1002/humu.20799. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
