

Revision of broken knee megaprostheses: new solution to old problems
- PMID: 20544320
- PMCID: PMC2947678
- DOI: 10.1007/s11999-010-1409-2
Revision of broken knee megaprostheses: new solution to old problems
Abstract
Background: Low-cost indigenous megaprostheses used in the developing world are prone to mechanical failure but the frequency and causes are not well established.
Questions/purposes: We retrospectively analyzed the causes of failure, particularly design, and suggest changes to reduce the breakage. We also report our experience with revision surgery.
Methods: We identified 28 breakages in 266 megaprosthetic knee arthroplasties performed between January 2000 and December 2006. Twenty-six breakages were revised to another prosthesis. The complications were studied and the function was evaluated. Prostheses were studied for failure by the computer-aided design program SolidWorks(®) and Hyperworks(®) for finite element analysis (FEA). Design improvements were performed based on these results.
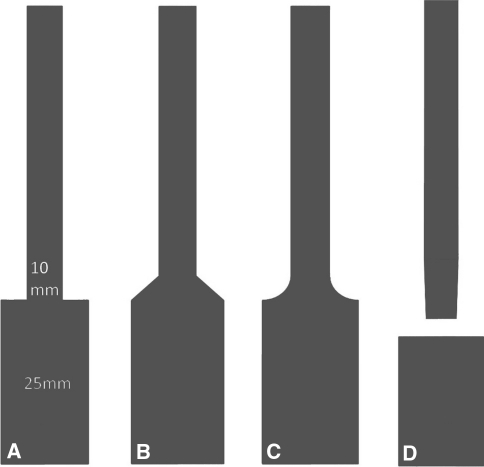
Results: In 21 cases, the failure occurred at the stem-collar junction, the point of maximum stress predicted by FEA. Stainless steel implants were prone to failure. There was one early and one late infection. Three patients died of metastatic disease. The most difficult surgical step involved the removal of the well-cemented broken stem from the intramedullary canal. Musculoskeletal Tumor Society scores varied from 27 to 29 after revision. FEA revealed stress could be reduced by filleting the stem-collar junction and by two-piece stems.
Conclusions: Revisions of broken total knee megaprostheses, though technically difficult, have allowed patients reasonable function. We recommend design analysis for custom prostheses to point to areas of weakness. Breakages can be reduced by using titanium stems and filleting the junction or by having two-piece inserted stems. Incorporating these changes has reduced the failures in our experience.
Figures






References
-
- Capanna R, Morris HG, Campanacci D, Del Ben M, Campanacci M. Modular uncemented prosthetic reconstruction after resection of tumours of the distal femur. J Bone Joint Surg Br. 1994;76:178–186. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
