

Out-of-hospital cardiac arrests occurring in southern Ontario health care clinics: bystander cardiopulmonary resuscitation and automated external defibrillator use
- PMID: 20547503
- PMCID: PMC2902391
Out-of-hospital cardiac arrests occurring in southern Ontario health care clinics: bystander cardiopulmonary resuscitation and automated external defibrillator use
Abstract
Objective: To determine the proportion of public-location out-of-hospital cardiac arrests (OHCAs) that occur in health care clinics and to describe bystander cardiopulmonary resuscitation (CPR) and automated external defibrillator (AED) use during these episodes.
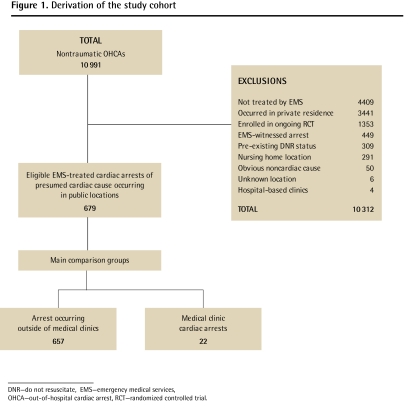
Design: Our study was a retrospective cohort study of 679 nontraumatic OHCAs recorded in the Resuscitation Outcomes Consortium Epistry-Cardiac Arrest database.
Setting: Out-of-hospital medical clinics and other public locations in Toronto, Ont, and the surrounding municipal regions of Hamilton, Durham, York, Peel, Simcoe, and Muskoka.
Participants: A total of 679 consecutive patients suffering nontraumatic OHCAs of presumed cardiac cause in public locations.
Main outcome measures: The proportion of public-location cardiac arrests occurring in medical clinics and the occurrence of bystander CPR and bystander use of AEDs.
Results: Twenty-two of the 679 public-location cardiac arrests occurred in health care clinics (3.2%, 95% confidence interval 1.9% to 4.6%). Bystander CPR occurred more often in health care clinics (73% of episodes in clinics compared with 46% in other public places, P = .02), but there was no statistically significant difference in AED use between groups. Twenty-seven percent of those suffering cardiac arrests in health care clinics did not receive any bystander CPR, and more than 90% did not have AEDs applied.
Conclusion: Although the response to cardiac arrest in out-of-hospital medical clinics is superior to the response to those arrests that occur in other public settings, it remains suboptimal. Increasing CPR training among staff and improving access to AEDs in medical clinics might improve the response to OHCA in medical clinics and ultimately improve outcomes for patients.
OBJECTIF: Établir la proportion des arrêts cardiaques extra-hospitaliers (ACEH) qui surviennent dans des cliniques de santé et décrire les manœuvres de ressuscitation cardiorespiratoires (RCR) et l’utilisation du défibrillateur externe automatique (DEA) durant ces épisodes.
TYPE D’ÉTUDE: Étude de cohorte rétrospective de 679 ACEH tirés de la base de données Ressuscitation Outcome Consortium Epistry-Cardiac Arrest.
CONTEXTE: Cliniques médicales extra-hospitalières et autres lieux publics de Toronto et des municipalités avoisinantes d’Hamilton, Durham, York, Peel, Simcoe et Muskoka, Ont.
PARTICIPANTS: Un total de 679 patients consécutifs ayant présenté un ACEH non traumatique de cause vraisemblablement cardiaque dans des lieux publics.
PRINCIPAUX PARAMÈTRES ÉTUDIÉS: La proportion des arrêts cardiaques des lieux publics survenant dans des cliniques médicales et les cas où les personnes présentes ont utilisé la RCR ou le DEA.
RÉSULTATS: Sur 679 arrêts cardiaques dans des lieux publics, 22 sont survenus dans des cliniques médicales (3,2 %, intervalle de confiance à 95 % 1,9 % à 4,6 %). Les manœuvres de RCR par les personnes présentes étaient plus fréquentes dans les cliniques médicales (73 % des épisodes dans les cliniques comparé à 46 % dans d’autres lieux publics, P = ,02), mais il n’y avait pas de différence significative entre les groupes pour l’utilisation du DEA. Parmi ceux qui ont eu un arrêt cardiaque dans des cliniques médicales, 27 % n’ont pas reçu de CPR par les personnes présentes et plus de 90 % n’ont pas subi demanoeuvres à l’aide d’un DEA.
CONCLUSION: Même si la réponse aux arrêts cardiaques dans les cliniques médicales extra-hospitalières est supérieure à celle observée quand l’arrêt survient dans d’autres lieux publics, elle demeure sous-optimale. Une formation en RCR accrue pour le personnel et un meilleur accès au DEA dans les cliniques médicales pourraient améliorer la réponse aux ACEH et ainsi améliorer les issues pour les patients.
Figures
References
-
- Stiell IG, Wells GA, Field B, Spaite DW, Nesbitt LP, De Maio VJ, et al. Advanced cardiac life support in out-of-hospital cardiac arrest. N Engl J Med. 2004;351(7):647–56. - PubMed
-
- Valenzuela TD, Roe DJ, Nichol G, Clark LL, Spaite DW, Hardman RG. Outcomes of rapid defibrillation by security officers after cardiac arrest in casinos. N Engl J Med. 2000;343(17):1206–9. - PubMed
-
- Holmberg M, Holmberg S, Herlitz J. Effect of bystander cardiopulmonary resuscitation in out-of-hospital cardiac arrest patients in Sweden. Resuscitation. 2000;47(1):59–70. - PubMed
-
- Stiell IG, Wells GA, Field BJ, Spaite DW, De Maio VJ, Ward R, et al. Improved out-of-hospital cardiac arrest survival through the inexpensive optimization of an existing defibrillation program: OPALS study phase II. Ontario Prehospital Advanced Life Support. JAMA. 1999;281(13):1175–81. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical