

Daily estimation of the severity of multiple organ dysfunction syndrome in critically ill children
- PMID: 20547715
- PMCID: PMC2917930
- DOI: 10.1503/cmaj.081715
Daily estimation of the severity of multiple organ dysfunction syndrome in critically ill children
Abstract
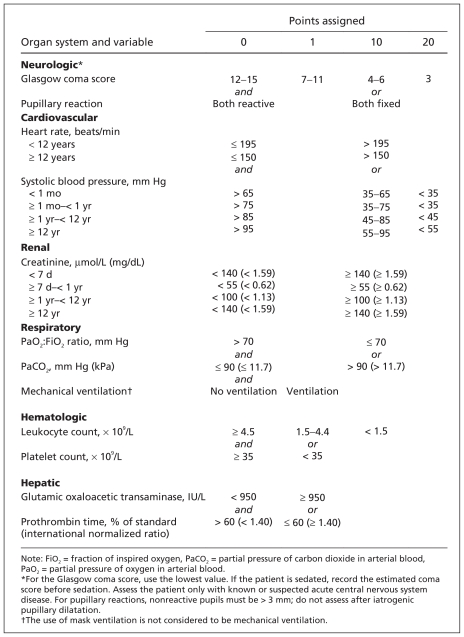
Background: Daily evaluation of multiple organ dysfunction syndrome has been performed in critically ill adults. We evaluated the clinical course of multiple organ dysfunction over time in critically ill children using the Pediatric Logistic Organ Dysfunction (PELOD) score and determined the optimal days for measuring scores.
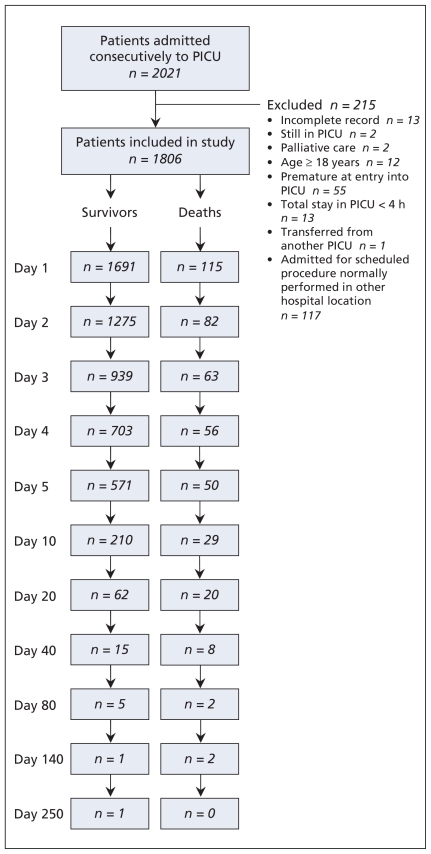
Methods: We prospectively measured daily PELOD scores and calculated the change in scores over time for 1806 consecutive patients admitted to seven pediatric intensive care units (PICUs) between September 1998 and February 2000. To study the relationship between daily scores and mortality in the PICU, we evaluated changes in daily scores during the first four days; the mean rate of change in scores during the entire PICU stay between survivors and nonsurvivors; and Cox survival analyses using a change in PELOD score as a time-dependent covariate to determine the optimal days for measuring daily scores.
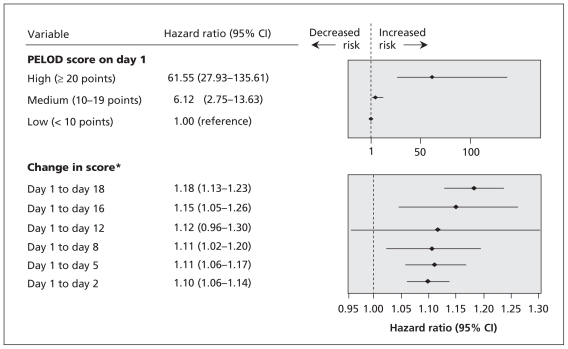
Results: The overall mortality among the 1806 patients was 6.4%. A high PELOD score (>or=20 points) on day 1 was associated with an odds ratio (OR) for death of 40.7 (95% confidence interval [CI] 20.3-81.4); a medium score (10-19 points) on day 1 was associated with an OR for death of 4.2 (95% CI 2.0-8.7). Mortality was 50% when a high score on day 1 increased on day 2. The course of daily PELOD scores differed between survivors and nonsurvivors. A set of seven days (days 1, 2, 5, 8, 12, 16 and 18) was identified as the optimal period for measurement of daily PELOD scores.
Interpretation: PELOD scores indicating a worsening condition or no improvement over time were indicators of a poor prognosis in the PICU. A set of seven days for measurement of the PELOD score during the PICU stay provided optimal information on the progression of multiple-organ dysfunction syndrome in critically ill children.
Figures
Comment in
-
Prognostic scoring in critically ill children: what to predict?CMAJ. 2010 Aug 10;182(11):1155-6. doi: 10.1503/cmaj.100553. Epub 2010 Jun 14. CMAJ. 2010. PMID: 20547709 Free PMC article. No abstract available.
References
-
- Cengiz P, Zimmerman JJ. Prelude to pediatric multiple organ dysfunction syndrome: the golden hours concept revisited. Pediatr Crit Care Med. 2003;4:263–4. - PubMed
-
- Marshall JC. Modeling MODS: What can be learned from animal models of the multiple-organ dysfunction syndrome? Intensive Care Med. 2005;31:605–8. - PubMed
-
- Proulx F, Gauthier M, Nadeau D, et al. Timing and predictors of death in pediatric patients with multiple organ system failure. Crit Care Med. 1994;22:1025–31. - PubMed
-
- Wilkinson JD, Pollack MM, Glass NL, et al. Mortality associated with multiple organ system failure and sepsis in pediatric intensive care unit. J Pediatr. 1987;111:324–8. - PubMed
-
- Tantalean JA, Leon RJ, Santos AA, et al. Multiple organ dysfunction syndrome in children. Pediatr Crit Care Med. 2003;4:181–5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources