

doi: 10.1128/AAC.01240-09.
Epub 2010 Jun 14.
Successful treatment for carriage of methicillin-resistant Staphylococcus aureus and importance of follow-up
Affiliations
- PMID: 20547792
- PMCID: PMC2934988
- DOI: 10.1128/AAC.01240-09
Item in Clipboard
Successful treatment for carriage of methicillin-resistant Staphylococcus aureus and importance of follow-up
Antimicrob Agents Chemother.
2010 Sep.
Abstract
With this prospective observational follow-up study of 165 methicillin-resistant Staphylococcus aureus (MRSA)-positive individuals (23 health care workers and 142 patients), we determined that our MRSA eradication therapy protocol results in a high success rate (81%). Five or more negative culture sets give a predictive value for MRSA eradication therapy success of >90%. Furthermore, MRSA colonization, at least in the throat, and the presence of wounds just before the start of MRSA eradication therapy are associated with MRSA eradication therapy failure.
Figures

Flowchart demonstrating the outcomes for MRSA-positive individuals after the first detection of MRSA. Unsuccessful treatment was defined as one or more cultures positive in one or more out of six consecutive follow-up culture sets (e.g., nose, throat, perineum, and any wounds or skin lesions present). *, patients not included because either (i) there was no treatment in our hospital (n, 26), (ii) they were not eligible for treatment (due to relative contraindications for eradication therapy, loss to follow-up after the first MRSA detection, or a high risk of noncompliance with treatment) (n, 17), or (iii) they died before treatment could be offered (n, 12). ¥, no new MRSA eradication therapy because of newly arisen relative contraindications for eradication therapy (n, 7), unavailability of new therapy in our hospital (n, 1); or loss to follow-up (n, 1). †, no new MRSA eradication therapy because of newly arisen relative contraindications for eradication therapy (n, 4). ‡, not included in the intention-to-treat analysis.
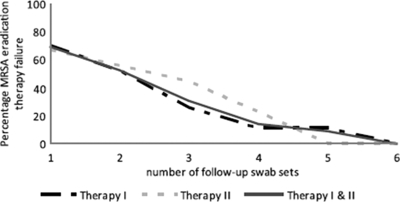
Number of MRSA-negative swabs needed to predict the success of MRSA eradication therapy as measured with 36 individuals whose MRSA eradication therapy failed.
References
-
- Adra, M., and K. R. Lawrence. 2004. Trimethoprim/sulfamethoxazole for treatment of severe Staphylococcus aureus infections. Ann. Pharmacother. 38:338-341. - PubMed
-
- Ammerlaan, H. S., J. A. Kluytmans, H. F. Wertheim, J. L. Nouwen, and M. J. Bonten. 2009. Eradication of methicillin-resistant Staphylococcus aureus carriage: a systematic review. Clin. Infect. Dis. 48:922-930. - PubMed
-
- Batra, R., A. C. Eziefula, D. Wyncoll, and J. Edgeworth. 2008. Throat and rectal swabs may have an important role in MRSA screening of critically ill patients. Intensive Care Med. 34:1703-1706. - PubMed
-
- Boyce, J. M. 1989. Methicillin-resistant Staphylococcus aureus. Detection, epidemiology, and control measures. Infect. Dis. Clin. North Am. 3:901-913. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
