

Screening for lung cancer with low-dose computed tomography: a systematic review and meta-analysis of the baseline findings of randomized controlled trials
- PMID: 20548246
- PMCID: PMC4006972
- DOI: 10.1097/JTO.0b013e3181e0b977
Screening for lung cancer with low-dose computed tomography: a systematic review and meta-analysis of the baseline findings of randomized controlled trials
Abstract
Objectives: Lung cancer is the leading cause of death among all cancers. An estimated 29% of the global population older than 15 years currently smokes tobacco. The presence of a high risk population, relatively asymptomatic nature of the disease in the early phase, and relatively good prognosis when discovered early makes screening for lung cancer an attractive proposition. We performed a systematic review and a meta-analysis of the baseline results of randomized controlled trials so far published, which included more than 14,000 patients. Analysis was used to determine whether data was for or against the screening of lung cancers using low-dose computed tomography (LDCT).
Design: Random effect meta regression model of meta-analysis and systematic review.
Methods: We performed a systematic review and a meta-analysis of the current literature to determine whether screening for lung cancer in a high-risk population with computed tomography improves outcomes. A search strategy using Medline was employed, studies selected based on preset criteria and application of exclusion criteria, and data collected and analyzed for statistical significance.
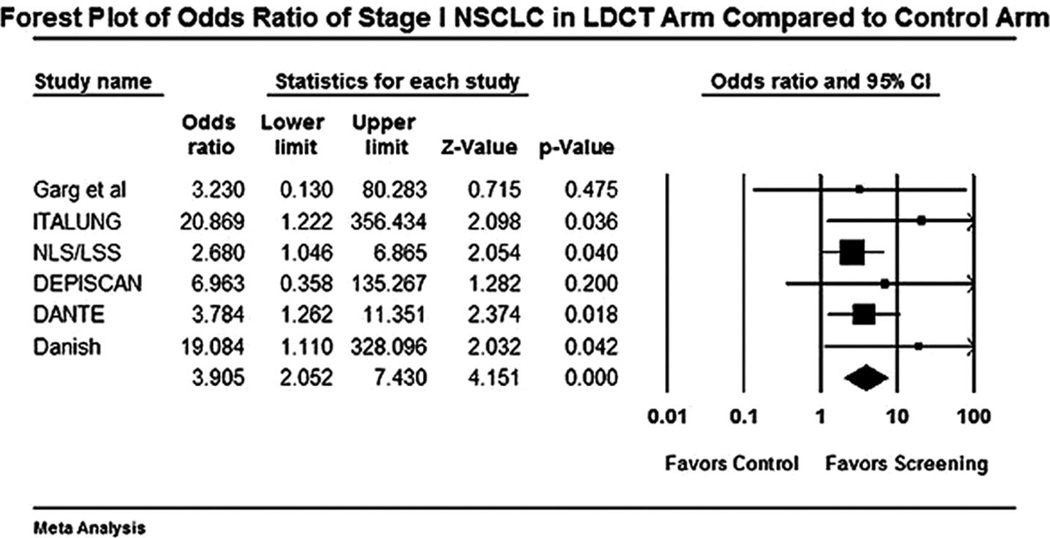
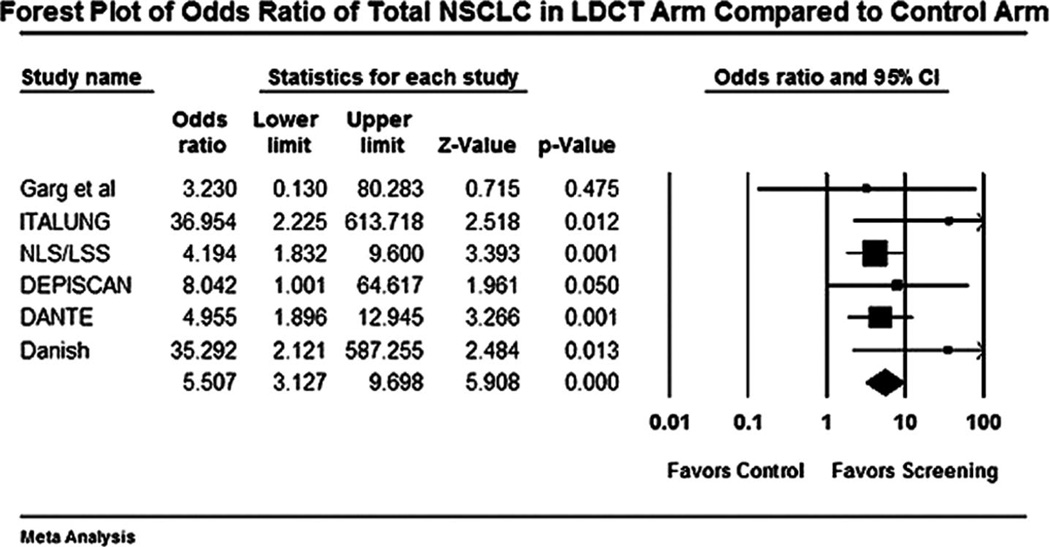
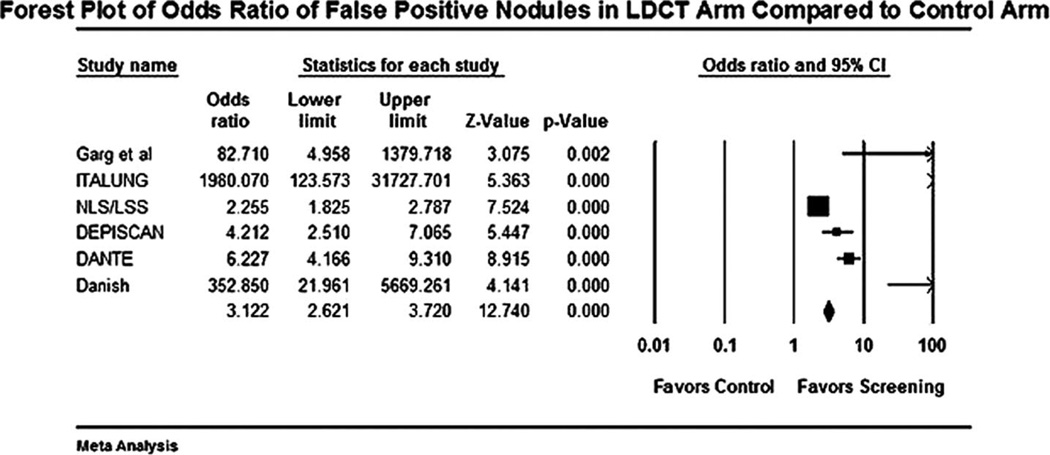
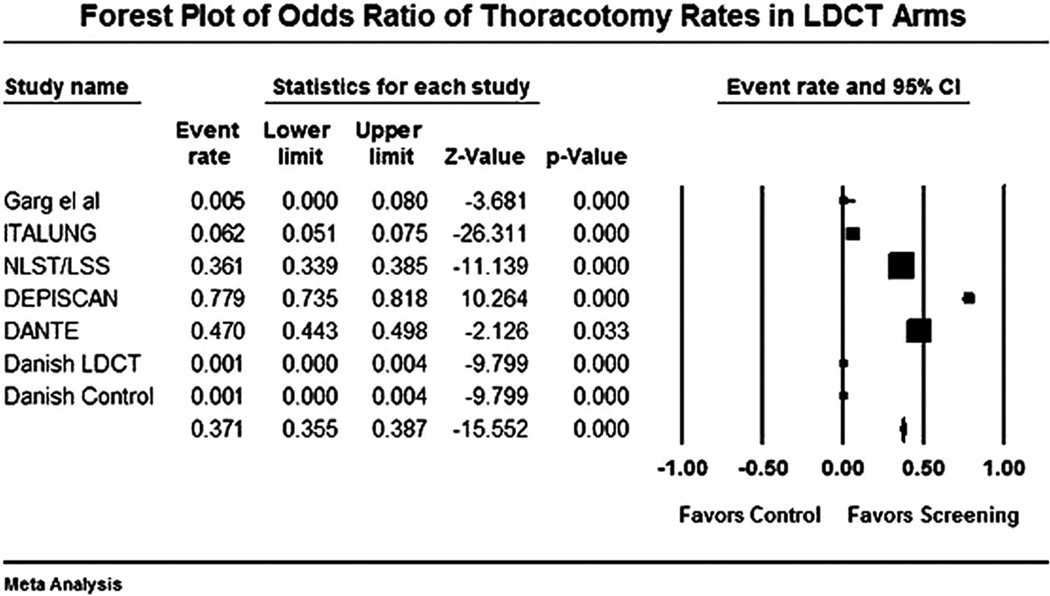
Results: Screening for lung cancer using LDCT resulted in a significantly higher number of stage I lung cancers (odds ratio 3.9, 95% confidence interval [CI] 2.0-7.4), higher number of total non-small cell lung cancers (odds ratio 5.5, 95% CI 3.1-9.6), and higher total lung cancers (odds ratio 4.1, 95% CI 2.4-7.1). Screening using LDCT also resulted in increased detection of false-positive nodules (odds ratio 3.1, 95% CI 2.6-3.7) and more unnecessary thoracotomies for benign lesions (event rate 3.7 per 1000, 95% CI 3.5-3.8). For every 1000 individuals screened with LDCT for lung cancer, 9 stage I non-small cell lung cancer and 235 false-positive nodules were detected, and 4 thoracotomies for benign lesions were performed.
Conclusions: The baseline data from six randomized controlled trials offer no compelling data in favor or against the use of LDCT screening for lung cancer. We await the final results of these randomized controlled trials to improve our understanding of the effectiveness of LDCT in the screening for lung cancer and its effect on mortality.
Conflict of interest statement
Disclosure: The authors declare no conflicts of interest.
Figures
References
-
- WHO. World Health Organization; 2009. Global Burden of Lung Cancer. Fact sheet No. 297.
-
- Cancer IAfRo. Worldwide Cancer Burden. World Cancer Report 2008. 2008:42–55.
-
- Flieder DB, Port JL, Korst RJ, et al. Tumor size is a determinant of stage distribution in t1 non-small cell lung cancer. Chest. 2005;128:2304–2308. - PubMed
-
- Henschke CI. Survival of patients with clinical stage I lung cancer diagnosed by computed tomography screening for lung cancer. Clin Cancer Res. 2007;13:4949–4950. - PubMed
-
- WHO. World Health Organization; 2007. Fact File: Tobacco and second-hand smoke.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
