

Decreases in community viral load are accompanied by reductions in new HIV infections in San Francisco
- PMID: 20548786
- PMCID: PMC2883572
- DOI: 10.1371/journal.pone.0011068
Decreases in community viral load are accompanied by reductions in new HIV infections in San Francisco
Abstract
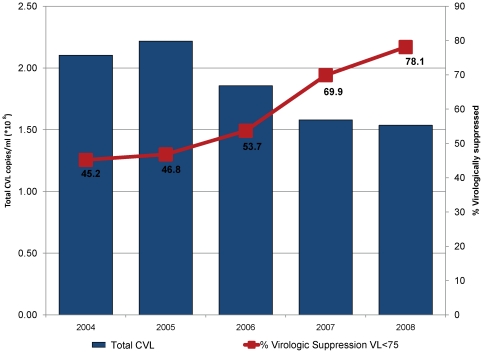
Background: At the individual level, higher HIV viral load predicts sexual transmission risk. We evaluated San Francisco's community viral load (CVL) as a population level marker of HIV transmission risk. We hypothesized that the decrease in CVL in San Francisco from 2004-2008, corresponding with increased rates of HIV testing, antiretroviral therapy (ART) coverage and effectiveness, and population-level virologic suppression, would be associated with a reduction in new HIV infections.
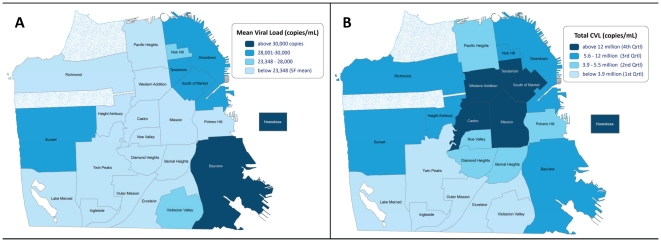
Methodology/principal findings: We used San Francisco's HIV/AIDS surveillance system to examine the trends in CVL. Mean CVL was calculated as the mean of the most recent viral load of all reported HIV-positive individuals in a particular community. Total CVL was defined as the sum of the most recent viral loads of all HIV-positive individuals in a particular community. We used Poisson models with robust standard errors to assess the relationships between the mean and total CVL and the primary outcome: annual numbers of newly diagnosed HIV cases. Both mean and total CVL decreased from 2004-2008 and were accompanied by decreases in new HIV diagnoses from 798 (2004) to 434 (2008). The mean (p = 0.003) and total CVL (p = 0.002) were significantly associated with new HIV cases from 2004-2008.
Conclusions/significance: Reductions in CVL are associated with decreased HIV infections. Results suggest that wide-scale ART could reduce HIV transmission at the population level. Because CVL is temporally upstream of new HIV infections, jurisdictions should consider adding CVL to routine HIV surveillance to track the epidemic, allocate resources, and to evaluate the effectiveness of HIV prevention and treatment efforts.
Conflict of interest statement
Figures
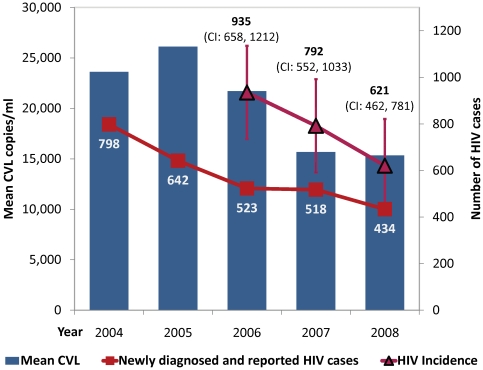
 ) decreased in San Francisco from 798 (2004) to 434 (2008) (p<0.005). The point estimates of HIV incidence (shown in dark red with ▵) using the CDC methods also declined from 935 [95% CI 658–1212] in 2006, to 792 [552–1033] in 2007 and 621 [462–781] in 2008, although the change was not statistically significant (trend p = 0.29). The reductions in annual measures of mean CVL were significantly associated with decreases in newly diagnosed and reported HIV cases from 2004–2008 (p = 0.003). Longitudinal reductions in estimated HIV incidence were consistent with the trends in mean and total CVL, but the association in the meta-regression was not statistically significant (p>0.3).
) decreased in San Francisco from 798 (2004) to 434 (2008) (p<0.005). The point estimates of HIV incidence (shown in dark red with ▵) using the CDC methods also declined from 935 [95% CI 658–1212] in 2006, to 792 [552–1033] in 2007 and 621 [462–781] in 2008, although the change was not statistically significant (trend p = 0.29). The reductions in annual measures of mean CVL were significantly associated with decreases in newly diagnosed and reported HIV cases from 2004–2008 (p = 0.003). Longitudinal reductions in estimated HIV incidence were consistent with the trends in mean and total CVL, but the association in the meta-regression was not statistically significant (p>0.3).References
-
- Garcia PM, Kalish LA, Pitt J, Minkoff H, Quinn TC, et al. Maternal levels of plasma human immunodeficiency virus type 1 RNA and the risk of perinatal transmission. Women and Infants Transmission Study Group. N Engl J Med. 1999;341:394–402. - PubMed
-
- HIV testing and prophylaxis to prevent mother-to-child transmission in the United States. Pediatrics. 2008;122:1127–1134. - PubMed
-
- Cooper ER, Charurat M, Mofenson L, Hanson IC, Pitt J, et al. Combination antiretroviral strategies for the treatment of pregnant HIV-1-infected women and prevention of perinatal HIV-1 transmission. J Acquir Immune Defic Syndr. 2002;29:484–494. - PubMed
-
- Dickover RE, Garratty EM, Herman SA, Sim MS, Plaeger S, et al. Identification of levels of maternal HIV-1 RNA associated with risk of perinatal transmission. Effect of maternal zidovudine treatment on viral load. Jama. 1996;275:599–605. - PubMed
-
- Mofenson LM, Lambert JS, Stiehm ER, Bethel J, Meyer WA, 3rd, et al. Risk factors for perinatal transmission of human immunodeficiency virus type 1 in women treated with zidovudine. Pediatric AIDS Clinical Trials Group Study 185 Team. N Engl J Med. 1999;341:385–393. - PubMed
