

Drug-eluting versus bare-metal stent for treatment of saphenous vein grafts: a meta-analysis
- PMID: 20548794
- PMCID: PMC2883580
- DOI: 10.1371/journal.pone.0011040
Drug-eluting versus bare-metal stent for treatment of saphenous vein grafts: a meta-analysis
Abstract
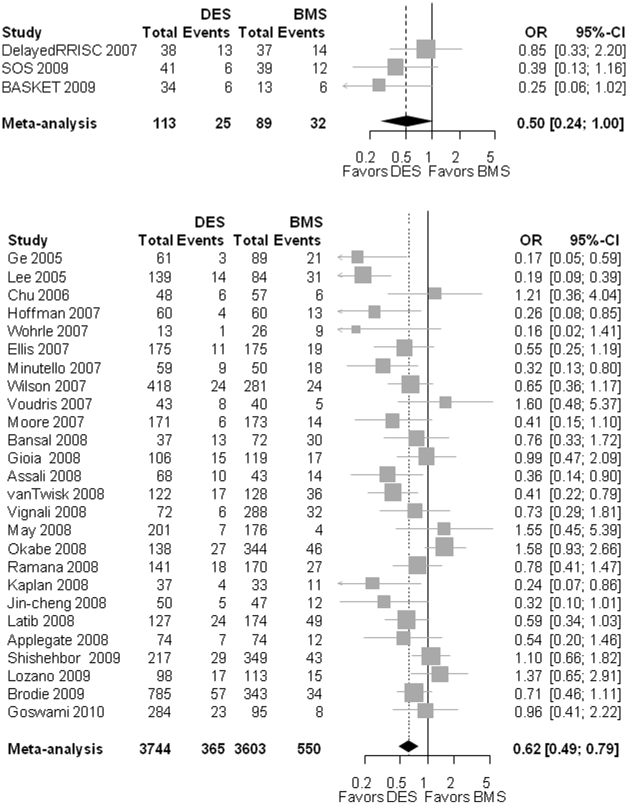
Background: Saphenous vein grafts develop an aggressive atherosclerotic process and the efficacy of drug eluting stents (DES) in treating saphenous vein graft (SVG) lesions has not been convincingly demonstrated. The aim of this study was to review and analyze the current literature for controlled studies comparing DES versus bare metal stents (BMS) for treatment of SVG stenoses.
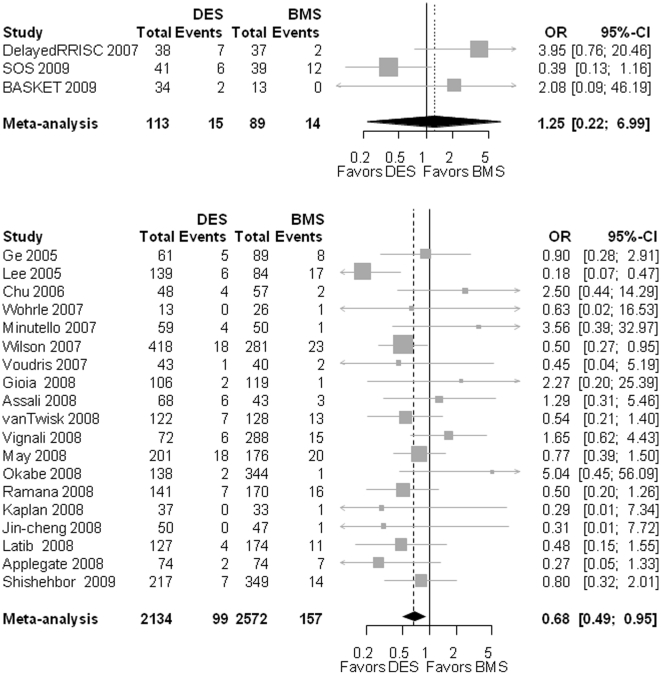
Methodology/principal findings: We searched several scientific databases and conference proceedings up to March 15, 2010 for controlled studies comparing target vessel revascularization (TVR) between DES and BMS. Summary odds ratios (OR) for the primary endpoint TVR and secondary endpoints infarction, stent thrombosis and death were calculated using random-effect models. A total of 29 studies (3 randomized controlled trials RCT) involving 7549 (202 in RCT) patients were included. The need for target vessel revascularization in the DES group tended to be lower compared to BMS for the 3 RCT (OR 0.50 [0.24-1.00]; p = 0.051) and for observational studies (0.62 [0.49-0.79]; p<0.001). There was no significant difference in the risk for myocardial infarction in the RCT (OR 1.25 [0.22-6.99]; p = 0.250) but a lower risk for DES based on the observational studies 0.68 [0.49-0.95]; p = 0.023. The risk for stent thrombosis was found to be non-different in the RCT (OR 0.78 [0.03-21.73], p = 0.885) while it was in favor of DES in the observational studies (0.58 [0.38 - 0.84]; p<0.001). The mortality was not significantly different between DES and BMS in the RCT's (OR 2.22 [0.17 - 29.50]; p = 0.546) while the observation studies showed a decreased mortality in the DES group (0.69 [0.55-0.85]; p<0.001).
Conclusion: DES may decrease TVR rate in treatment of SVG stenoses. No differences in reinfarction rate, stent thrombosis or mortality was found between the DES and BMS groups in the RCT's while the observational data showed lower risk for myocardial infarction, stent thrombosis and death in the DES group. This may be a result of patient selection bias in the observational studies or represent a true finding that was not the detected in the RCT analysis due to limited statistical power.
Conflict of interest statement
Figures



Similar articles
-
Drug-Eluting Versus Bare Metal Stents in Saphenous Vein Graft Intervention: An Updated Comprehensive Meta-Analysis of Randomized Trials.Cardiovasc Revasc Med. 2019 Sep;20(9):758-767. doi: 10.1016/j.carrev.2018.11.013. Epub 2018 Nov 22. Cardiovasc Revasc Med. 2019. PMID: 30503811
-
Drug eluting versus bare metal stents for percutaneous coronary intervention of saphenous vein graft lesions: An updated meta-analysis of randomized controlled trials.Cardiovasc Revasc Med. 2018 Oct-Nov;19(7 Pt B):837-844. doi: 10.1016/j.carrev.2018.03.025. Epub 2018 Apr 3. Cardiovasc Revasc Med. 2018. PMID: 29685385
-
The short- and long-term outcomes of percutaneous intervention with drug-eluting stent vs bare-metal stent in saphenous vein graft disease: An updated meta-analysis of all randomized clinical trials.Clin Cardiol. 2018 May;41(5):685-692. doi: 10.1002/clc.22908. Epub 2018 May 11. Clin Cardiol. 2018. PMID: 29749621 Free PMC article. Review.
-
Outcomes with drug-eluting versus bare-metal stents in saphenous vein graft intervention results from the STENT (strategic transcatheter evaluation of new therapies) group.JACC Cardiovasc Interv. 2009 Nov;2(11):1105-12. doi: 10.1016/j.jcin.2009.08.020. JACC Cardiovasc Interv. 2009. PMID: 19926052
-
Safety and efficacy of drug-eluting stents versus bare-metal stents in saphenous vein grafts lesions: a meta-analysis.EuroIntervention. 2010 May;6(1):149-60. EuroIntervention. 2010. PMID: 20542811 Review.
Cited by
-
Current State of the Art in Approaches to Saphenous Vein Graft Interventions.Interv Cardiol. 2017 Sep;12(2):85-91. doi: 10.15420/icr.2017:4:2. Interv Cardiol. 2017. PMID: 29588735 Free PMC article.
-
Management and Prevention of Saphenous Vein Graft Failure: A Review.Cardiol Ther. 2017 Dec;6(2):203-223. doi: 10.1007/s40119-017-0094-6. Epub 2017 Jul 26. Cardiol Ther. 2017. PMID: 28748523 Free PMC article. Review.
-
[No title available]Acta Cardiol Sin. 2014 Sep;30(5):485-9. Acta Cardiol Sin. 2014. PMID: 27122823 Free PMC article.
-
An update on coronary bypass graft intervention.Heart Asia. 2014 Mar 6;6(1):41-5. doi: 10.1136/heartasia-2013-010478. eCollection 2014. Heart Asia. 2014. PMID: 27326165 Free PMC article. Review.
-
Management of Saphenous Vein Graft Disease in Patients with Prior Coronary Artery Bypass Surgery.Curr Treat Options Cardiovasc Med. 2019 Feb 28;21(2):12. doi: 10.1007/s11936-019-0714-7. Curr Treat Options Cardiovasc Med. 2019. PMID: 30820682 Review.
References
-
- Wilson CT, Fisher ES, Welch HG, Siewers AE, Lucas FL. U.S. trends in CABG hospital volume: the effect of adding cardiac surgery programs. Health Aff (Millwood) 2007;26:162–168. - PubMed
-
- Brilakis ES, Wang TY, Rao SV, Banerjee S, Dai D, et al. 2010. Frequency and Predictors of Drug-Eluting Stent Use in Saphenous Vein Bypass Graft Percutaneous Coronary Interventions: A Report from the American College of Cardiology - National Cardiovascular Data Registry (abstract). presented at American College of Cardiology ACC scientific meetings 2010, March 14; Atlanta, Georgia.
-
- Rodes-Cabau J, Bertrand OF, Larose E, Dery JP, Rinfret S, et al. Comparison of plaque sealing with paclitaxel-eluting stents versus medical therapy for the treatment of moderate nonsignificant saphenous vein graft lesions: the moderate vein graft lesion stenting with the taxus stent and intravascular ultrasound (VELETI) pilot trial. Circulation. 2009;120:1978–1986. - PubMed
-
- Tonino PA, De Bruyne B, Pijls NH, Siebert U, Ikeno F, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009;360:213–224. - PubMed
-
- Safian RD. Accelerated atherosclerosis in saphenous vein bypass grafts: a spectrum of diffuse plaque instability. Prog Cardiovasc Dis. 2002;44:437–448. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
