

Intraosseous ameloblastoma with a prominent extraosseous component: pitfalls in diagnosis
- PMID: 20549402
- PMCID: PMC2923316
- DOI: 10.1007/s12105-010-0182-6
Intraosseous ameloblastoma with a prominent extraosseous component: pitfalls in diagnosis
Abstract
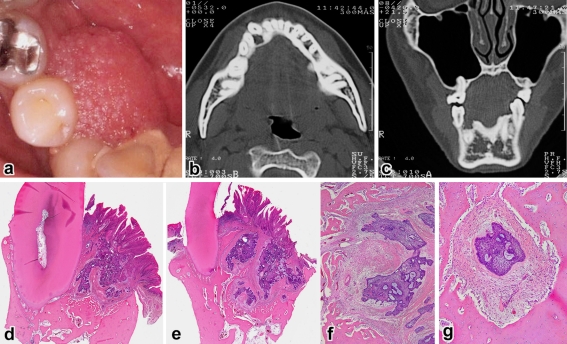
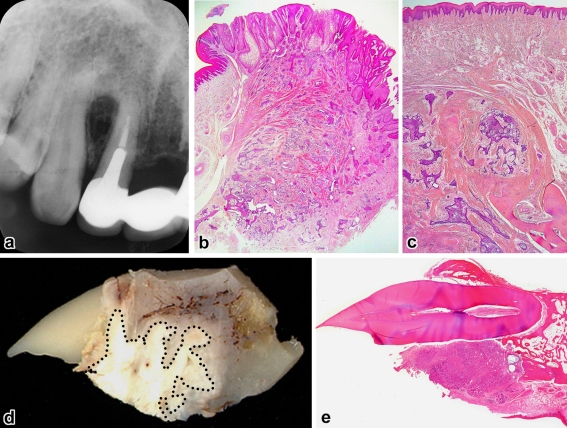
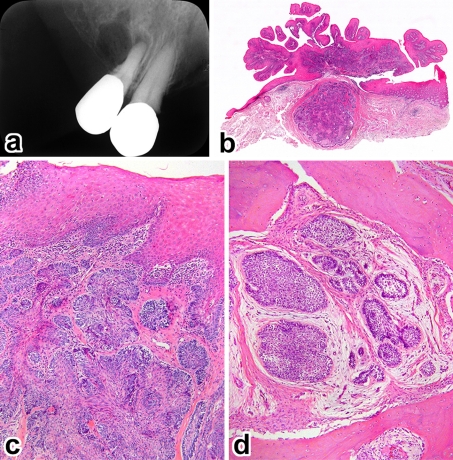
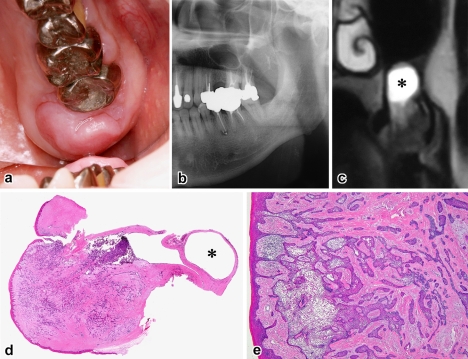
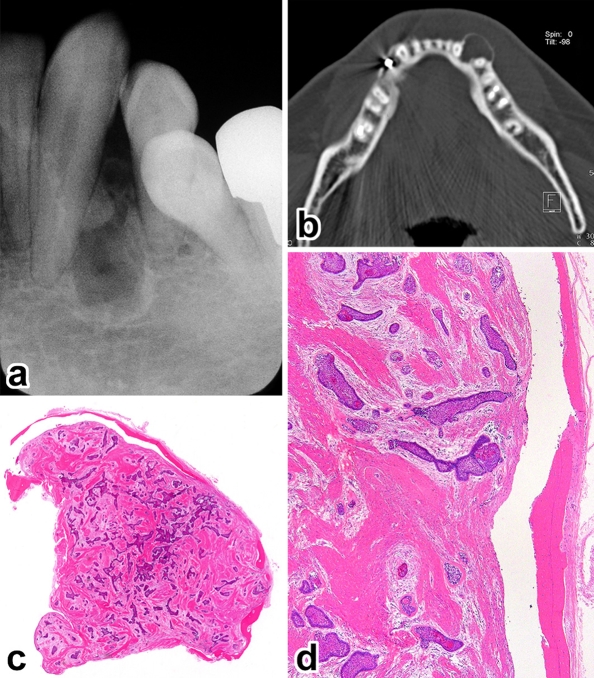
For many years, gingival tumors of what appear to be peripherally located intraosseous ameloblastoma (IA) arising from the alveolar bone surface have often been confused with peripheral ameloblastoma (PA) causing resorption of the underlying bone. We analyzed a series of five cases of ameloblastoma that demonstrated a combined PA and IA architecture. The tumor commonly involved the anterior-premolar area, mostly in the maxilla and mainly in middle-aged men. The clinical presentation was an exophytic gingival mass inferior to which was a small bone defect. The predominant extraosseous component showed a papillary gross surface, reflecting the histologic proof of fusion between the submucosal tumor and the surface epithelium. In addition to the PA-like growth pattern, common to all was the presence of neoplastic destruction of the alveolar process, corresponding to an associated radiolucent lesion. This restrained component was acceptable as IA. In two cases, recurrence was observed deep in the alveolar bone with no involvement of the gingiva. These tumors appear to be IA that arose from the marginal alveolar bone and grew preferentially in the gingiva, forming a PA-like appearance. From diagnostic, therapeutic and prognostic points of view, this type of IA should not be confused with PA.
Figures
Similar articles
-
[Diagnosis and therapy of ameloblastoma].Minerva Stomatol. 1984 Sep-Oct;33(5):827-40. Minerva Stomatol. 1984. PMID: 6394986 Italian. No abstract available.
-
Unicystic ameloblastoma: a clinicopathologic study of 33 Chinese patients.Am J Surg Pathol. 2000 Oct;24(10):1385-92. doi: 10.1097/00000478-200010000-00008. Am J Surg Pathol. 2000. PMID: 11023100
-
Ameloblastoma in the maxillomandibular region: MR imaging.Radiology. 1992 Aug;184(2):389-93. doi: 10.1148/radiology.184.2.1620834. Radiology. 1992. PMID: 1620834
-
Pulmonary metastasectomy in the treatment of recurrent ameloblastoma of the maxilla and mandible: a case report.Eur Arch Otorhinolaryngol. 2001 Jan;258(1):25-7. doi: 10.1007/s004050000293. Eur Arch Otorhinolaryngol. 2001. PMID: 11271430 Review.
-
Peripheral ameloblastoma: biological profile based on 160 cases from the literature.Oral Oncol. 2001 Jan;37(1):17-27. doi: 10.1016/s1368-8375(00)00064-6. Oral Oncol. 2001. PMID: 11120479 Review.
Cited by
-
P63 and Ki-67 Expression in Dentigerous Cyst and Ameloblastomas.J Dent (Shiraz). 2015 Dec;16(4):323-8. J Dent (Shiraz). 2015. PMID: 26636120 Free PMC article.
-
Peripheral ameloblastoma with neoplastic osseous invasion versus peripheral intraosseous ameloblastoma: A challenging diagnosis.J Oral Maxillofac Pathol. 2018 Sep-Dec;22(3):396-400. doi: 10.4103/jomfp.JOMFP_130_17. J Oral Maxillofac Pathol. 2018. PMID: 30651686 Free PMC article.
-
Atypical periosteal reaction and unusual bone involvement of ameloblastoma: A case report with 8-year follow-up.Imaging Sci Dent. 2021 Jun;51(2):195-201. doi: 10.5624/isd.20200264. Epub 2021 Jan 29. Imaging Sci Dent. 2021. PMID: 34235065 Free PMC article.
References
-
- Gardner DG, Heikinheimo K, Shear M, Philipsen HP, Coleman H. Ameloblastomas. In: Barnes L, Eveson JW, Reichart P, Sidransky D, editors. Pathology and genetics of head and neck tumours. Lyon: IARC Press; 2005. pp. 296–300.
-
- Jordan RCK, Speight PM. Current concepts of odontogenic tumours. Diagn Histopathol. 2009;15:303–310. doi: 10.1016/j.mpdhp.2009.03.002. - DOI
-
- Waal I, Rijcke TBM, Kwast WAM. Possible squamous odontogenic tumor: report of case. J Oral Surg. 1980;38:460–462. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
