

A prospective study of aromatase inhibitor-associated musculoskeletal symptoms and abnormalities on serial high-resolution wrist ultrasonography
- PMID: 20549827
- PMCID: PMC2936686
- DOI: 10.1002/cncr.25385
A prospective study of aromatase inhibitor-associated musculoskeletal symptoms and abnormalities on serial high-resolution wrist ultrasonography
Abstract
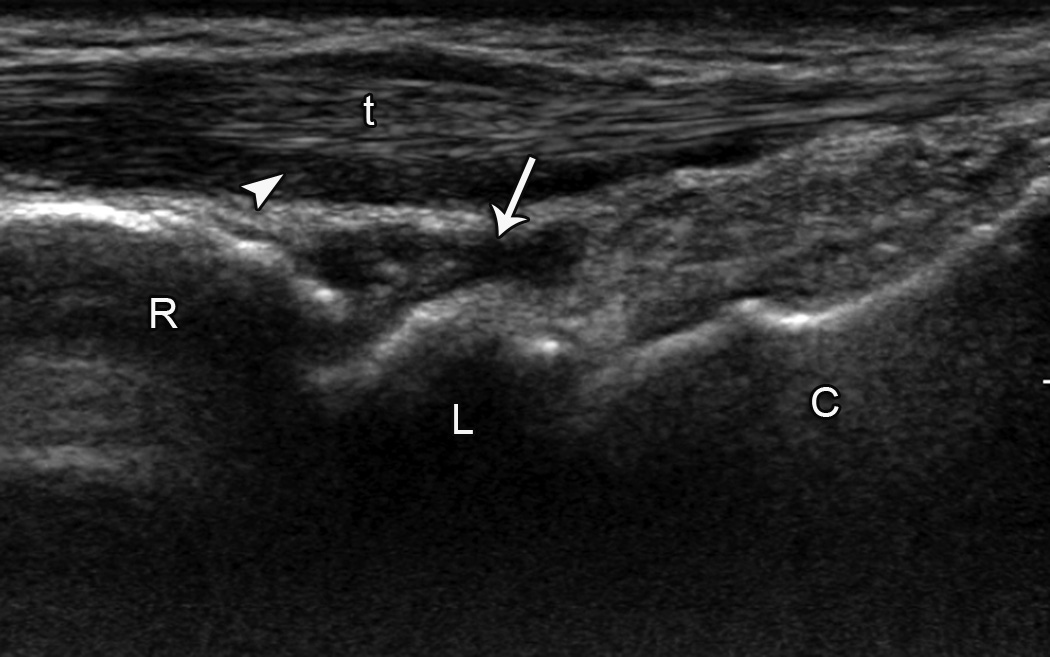
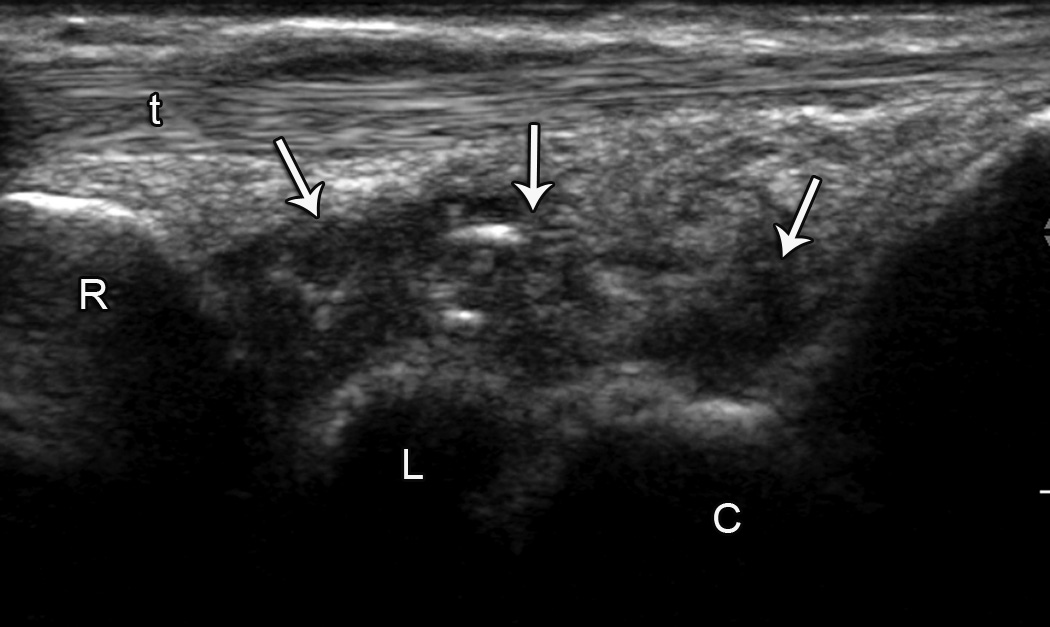
Background: Nearly half of women treated with aromatase inhibitors (AI) develop AI-associated musculoskeletal symptoms (AIMSS) such as arthralgias, but to the authors' knowledge the etiology is unclear. The upper extremities are frequently affected, especially the wrists, hands, and fingers. AI use may also increase the risk of developing carpal tunnel syndrome. Tendon sheath fluid and tenosynovial changes have been demonstrated by imaging symptomatic patients who were treated with AIs. The authors hypothesized that these abnormalities are correlated with AIMSS.
Methods: Thirty consecutive patients in whom adjuvant therapy with letrozole or exemestane was initiated on a prospective clinical trial enrolled in a pilot study evaluating tendon and joint abnormalities at baseline and after 3 months of AI therapy. Patients underwent high-resolution ultrasonography of the wrists bilaterally and completed the Health Assessment Questionnaire (HAQ) and pain Visual Analog Scale (VAS). AIMSS were defined as an increase in the HAQ or VAS score during AI therapy that exceeded a predefined cutoff.
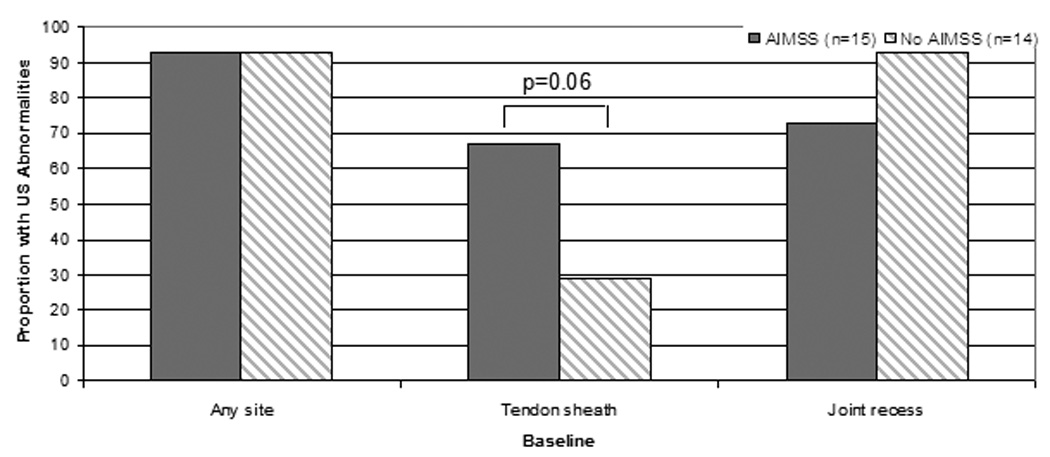
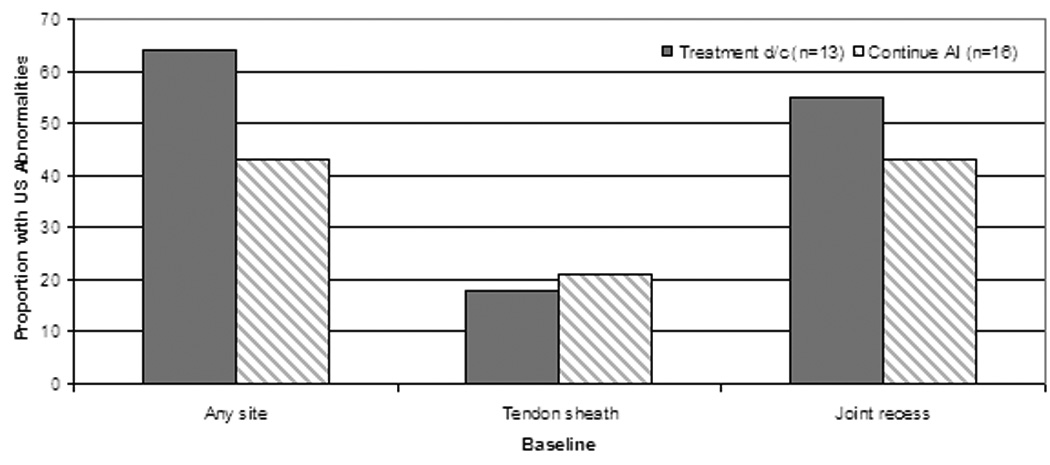
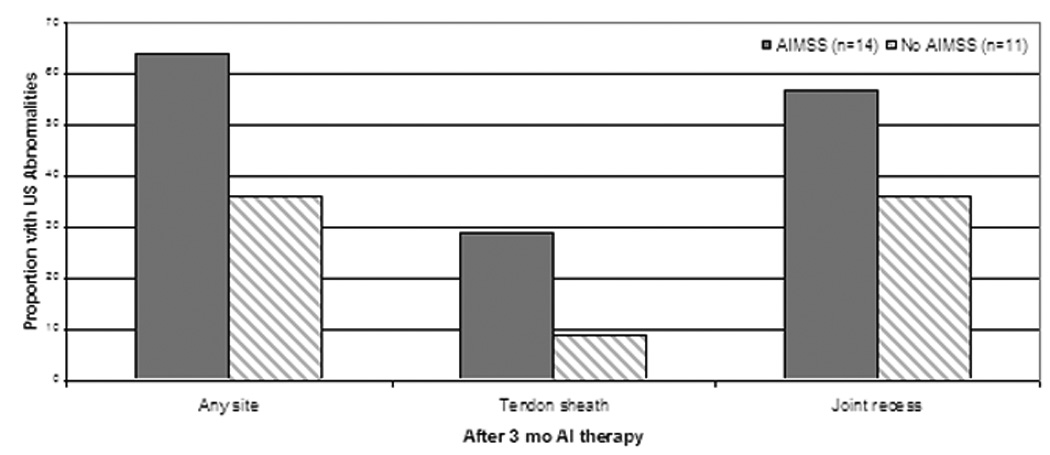
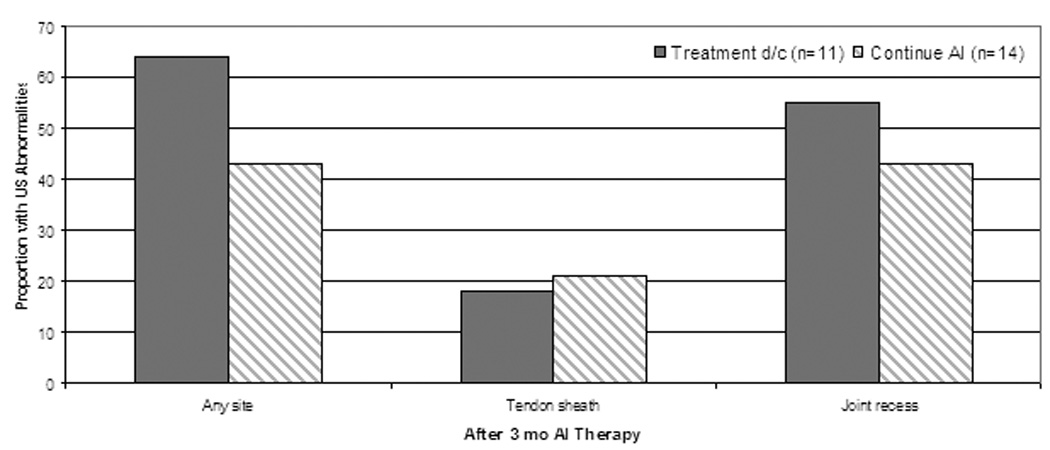
Results: Twenty-five patients completed both the baseline and 3-month assessments. During the first 12 months of AI therapy, 15 patients developed AIMSS, and 13 discontinued therapy because of musculoskeletal symptoms. There was a trend toward an association between the presence of tendon sheath abnormalities on wrist ultrasound at baseline and the development of AIMSS (P = .06).
Conclusions: Clinically relevant musculoskeletal symptoms develop in women treated with AIs, leading to treatment discontinuation in a substantial percentage of these patients. However, in the current study, patient-reported symptoms were not found to be associated with changes visible on wrist ultrasonography.
Trial registration: ClinicalTrials.gov NCT00228956.
© 2010 American Cancer Society.
Figures
References
-
- Forbes JF, Cuzick J, Buzdar A, Howell A, Tobias JS, Baum M. Effect of anastrozole and tamoxifen as adjuvant treatment for early-stage breast cancer: 100-month analysis of the ATAC trial. Lancet Oncol. 2008;9:45–53. - PubMed
-
- Boccardo F, Rubagotti A, Puntoni M, Guglielmini P, Amoroso D, Fini A, et al. Switching to anastrozole versus continued tamoxifen treatment of early breast cancer: preliminary results of the Italian Tamoxifen Anastrozole trial. J Clin Oncol. 2005;23:5138–5147. - PubMed
-
- Coombes RC, Kilburn LS, Snowdon CF, Paridaens R, Coleman RE, Jones SE, et al. Survival and safety of exemestane versus tamoxifen after 2–3 years' tamoxifen treatment (Intergroup Exemestane Study): a randomised controlled trial. Lancet. 2007;369:559–570. - PubMed
-
- Goss PE, Ingle JN, Martino S, Robert NJ, Muss HB, Piccart MJ, et al. Randomized trial of letrozole following tamoxifen as extended adjuvant therapy in receptor-positive breast cancer: updated findings from NCIC CTG MA. 17. J Natl Cancer Inst. 2005;97:1262–1271. - PubMed
-
- Winer EP, Hudis C, Burstein HJ, Wolff AC, Pritchard KI, Ingle JN, et al. American Society of Clinical Oncology technology assessment on the use of aromatase inhibitors as adjuvant therapy for postmenopausal women with hormone receptor-positive breast cancer: status report 2004. J Clin Oncol. 2005;23:619–629. - PubMed
