

Methodologic evaluation of adaptive conjoint analysis to assess patient preferences: an application in oncology
- PMID: 20550594
- PMCID: PMC5060551
- DOI: 10.1111/j.1369-7625.2010.00595.x
Methodologic evaluation of adaptive conjoint analysis to assess patient preferences: an application in oncology
Abstract
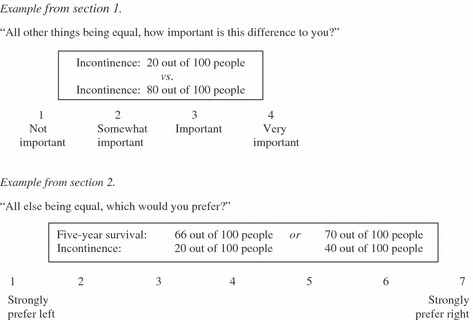
Background: Adaptive conjoint analysis (ACA) is an individually tailored preferences elicitation technique that mimics actual decision-making processes by asking participants to make trade-offs between the various dimensions that underlie decision problems. ACA is increasingly applied in patient preferences assessments but formal evaluation of its validity and reliability is lacking.
Objective: To investigate ACA's validity and reliability in elicitation of treatment outcome preferences.
Methods: Sixty-eight disease-free rectal cancer patients, treated with surgery with or without preoperative radiotherapy were asked to complete exercises to assess their preferences for radiotherapy [using the treatment trade-off method (TTM)] and for key outcomes associated with radiotherapy (using ACA). We assessed (i) rank ordering of ACA-derived outcome-probability utilities, (ii) compensatory decision making, (iii) ACA test-retest reliability, and (iv) concordance of ACA- and TTM-based preferences.
Results: All participants completed the TTM and 66 completed the ACA questionnaire, in 15 min on average. Outcome utilities were rank ordered in agreement with probabilities from best to worst in most participants, except for sexual dysfunction. Most participants were willing to trade survival and their most important outcome. Mean importance ratings were similar at retest. ACA- and TTM-based preferences differed. TTM-based preferences were related to past treatment, ACA-based preferences were not.
Conclusions: ACA assesses group-level preferences reliably over time and captures individual preferences independently from treatment experience in treated cancer patients. ACA seems a valid treatment outcome preference elicitation method in a context in which trade-offs between cure and quality of life need to be considered.
© 2010 The Authors. Health Expectations © 2010 Blackwell Publishing Ltd.
Figures
Similar articles
-
Adaptive Conjoint Analysis as individual preference assessment tool: feasibility through the internet and reliability of preferences.Patient Educ Couns. 2010 Feb;78(2):224-33. doi: 10.1016/j.pec.2009.05.020. Epub 2009 Jul 5. Patient Educ Couns. 2010. PMID: 19581069
-
Benefit from preoperative radiotherapy in rectal cancer treatment: disease-free patients' and oncologists' preferences.Br J Cancer. 2007 Sep 17;97(6):717-24. doi: 10.1038/sj.bjc.6603954. Br J Cancer. 2007. PMID: 17848910 Free PMC article.
-
Patient explicit consideration of tradeoffs in decision making about rectal cancer treatment: benefits for decision process and quality of life.Acta Oncol. 2019 Jul;58(7):1069-1076. doi: 10.1080/0284186X.2019.1594363. Epub 2019 Apr 11. Acta Oncol. 2019. PMID: 30971150
-
Individual Value Clarification Methods Based on Conjoint Analysis: A Systematic Review of Common Practice in Task Design, Statistical Analysis, and Presentation of Results.Med Decis Making. 2018 Aug;38(6):746-755. doi: 10.1177/0272989X18765185. Epub 2018 Mar 29. Med Decis Making. 2018. PMID: 29592585 Free PMC article.
-
Eliciting public preferences for healthcare: a systematic review of techniques.Health Technol Assess. 2001;5(5):1-186. doi: 10.3310/hta5050. Health Technol Assess. 2001. PMID: 11262422
Cited by
-
Empowering patients in decision-making in radiation oncology - can we do better?Mol Oncol. 2020 Jul;14(7):1442-1460. doi: 10.1002/1878-0261.12675. Epub 2020 Apr 13. Mol Oncol. 2020. PMID: 32198967 Free PMC article. Review.
-
Patient choice in colorectal cancer treatment - A systematic review and narrative synthesis of attribute-based stated preference studies.Colorectal Dis. 2022 Nov;24(11):1295-1307. doi: 10.1111/codi.16242. Epub 2022 Jul 18. Colorectal Dis. 2022. PMID: 35776854 Free PMC article.
-
Optimal Time Intervals between Pre-Operative Radiotherapy or Chemoradiotherapy and Surgery in Rectal Cancer?Front Oncol. 2014 Apr 7;4:50. doi: 10.3389/fonc.2014.00050. eCollection 2014. Front Oncol. 2014. PMID: 24778990 Free PMC article. Review.
-
Use of Conjoint Analysis to Determine Patient Preferences for Surgical Treatment of Urethral Stricture Disease.J Particip Med. 2017;9:e1. Epub 2017 Jan 14. J Particip Med. 2017. PMID: 32995067 Free PMC article.
-
Effectiveness of a Decision Aid Plus Standard Care in Surgical Management Among Patients With Early Breast Cancer: A Randomized Clinical Trial.JAMA Netw Open. 2023 Oct 2;6(10):e2335941. doi: 10.1001/jamanetworkopen.2023.35941. JAMA Netw Open. 2023. PMID: 37782500 Free PMC article. Clinical Trial.
References
-
- Sepucha K, Ozanne E, Mulley AG Jr. Doing the right thing: systems support for decision quality in cancer care. Annals of Behavioral Medicine, 2006; 32: 172–178. - PubMed
-
- Hlatky MA. Patient preferences and clinical guidelines. JAMA, 1995; 273: 1219–1220. - PubMed
-
- Brothers TE, Cox MH, Robison JG, Elliott BM, Nietert P. Prospective decision analysis modeling indicates that clinical decisions in vascular surgery often fail to maximize patient expected utility. The Journal of Surgical Research, 2004; 120: 278–287. - PubMed
-
- Cotler SJ, Patil R, McNutt RA et al. Patients’ values for health states associated with hepatitis C and physicians’ estimates of those values. The American Journal of Gastroenterology, 2001; 96: 2730–2736. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
