

Improvements in access to malaria treatment in Tanzania following community, retail sector and health facility interventions -- a user perspective
- PMID: 20550653
- PMCID: PMC2910017
- DOI: 10.1186/1475-2875-9-163
Improvements in access to malaria treatment in Tanzania following community, retail sector and health facility interventions -- a user perspective
Abstract
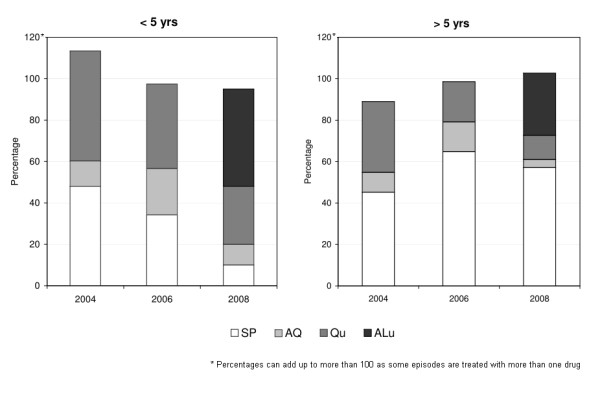
Background: The ACCESS programme aims at understanding and improving access to prompt and effective malaria treatment. Between 2004 and 2008 the programme implemented a social marketing campaign for improved treatment-seeking. To improve access to treatment in the private retail sector a new class of outlets known as accredited drug dispensing outlets (ADDO) was created in Tanzania in 2006. Tanzania changed its first-line treatment for malaria from sulphadoxine-pyrimethamine (SP) to artemether-lumefantrine (ALu) in 2007 and subsidized ALu was made available in both health facilities and ADDOs. The effect of these interventions on understanding and treatment of malaria was studied in rural Tanzania. The data also enabled an investigation of the determinants of access to treatment.
Methods: Three treatment-seeking surveys were conducted in 2004, 2006 and 2008 in the rural areas of the Ifakara demographic surveillance system (DSS) and in Ifakara town. Each survey included approximately 150 people who had suffered a fever case in the previous 14 days.
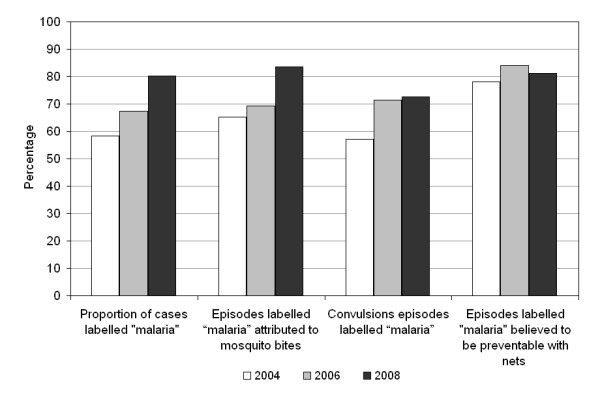
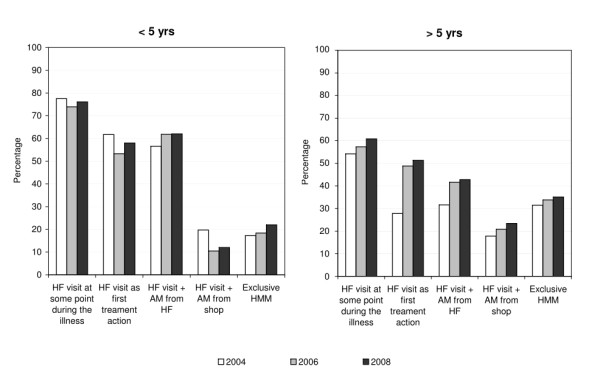
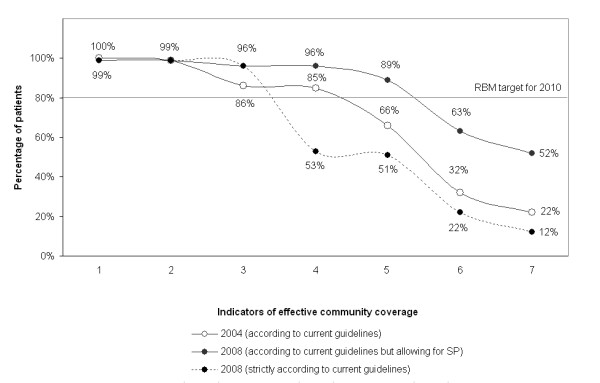
Results: Treatment-seeking and awareness of malaria was already high at baseline, but various improvements were seen between 2004 and 2008, namely: better understanding causes of malaria (from 62% to 84%); an increase in health facility attendance as first treatment option for patients older than five years (27% to 52%); higher treatment coverage with anti-malarials (86% to 96%) and more timely use of anti-malarials (80% to 93-97% treatments taken within 24 hrs). Unfortunately, the change of treatment policy led to a low availability of ALu in the private sector and, therefore, to a drop in the proportion of patients taking a recommended malaria treatment (85% to 53%). The availability of outlets (health facilities or drug shops) is the most important determinant of whether patients receive prompt and effective treatment, whereas affordability and accessibility contribute to a lesser extent.
Conclusions: An integrated approach aimed at improving understanding and treatment of malaria has led to tangible improvements in terms of people's actions for the treatment of malaria. However, progress was hindered by the low availability of the first-line treatment after the switch to ACT.
Figures
References
-
- World Health Organization. World Malaria Report 2009. Geneva. 2009.
-
- Roll Back Malaria. The Global Malaria Action Plan. Geneva. 2008.
-
- Smith LA, Jones C, Meek S, Webster J. Provider practice and user behavior interventions to improve prompt and effective treatment of malaria: do we know what works? Am J Trop Med Hyg. 2009;80:326–335. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
