

In-hospital percentage BNP reduction is highly predictive for adverse events in patients admitted for acute heart failure: the Italian RED Study
- PMID: 20550660
- PMCID: PMC2911763
- DOI: 10.1186/cc9067
In-hospital percentage BNP reduction is highly predictive for adverse events in patients admitted for acute heart failure: the Italian RED Study
Abstract
Introduction: Our aim was to evaluate the role of B-type natriuretic peptide (BNP) percentage variations at 24 hours and at discharge compared to its value at admission in order to demonstrate its predictive value for outcomes in patients with acute decompensated heart failure (ADHF).
Methods: This was a multicenter Italian (8 centers) observational study (Italian Research Emergency Department: RED). 287 patients with ADHF were studied through physical exams, lab tests, chest X Ray, electrocardiograms (ECGs) and BNP measurements, performed at admission, at 24 hours, and at discharge. Follow up was performed 180 days after hospital discharge. Logistic regression analysis was used to estimate odds ratios (OR) for the various subgroups created. For all comparisons, a P value < 0.05 was considered statistically significant.
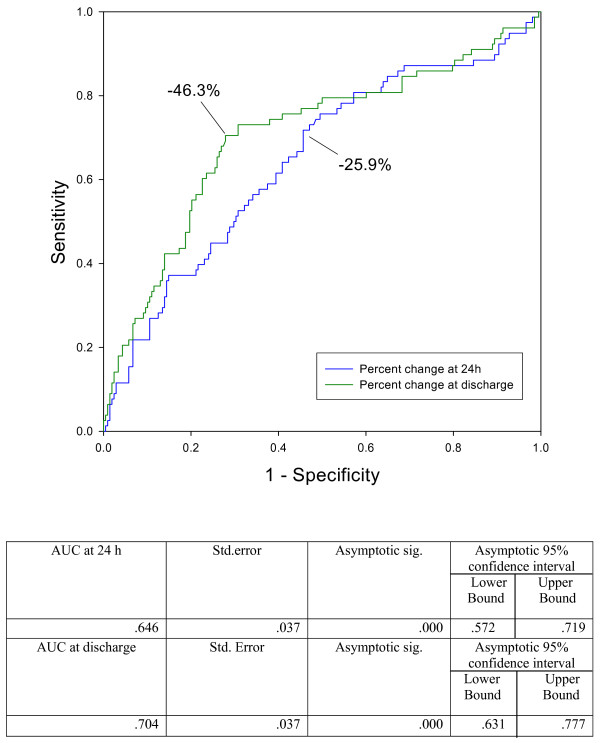
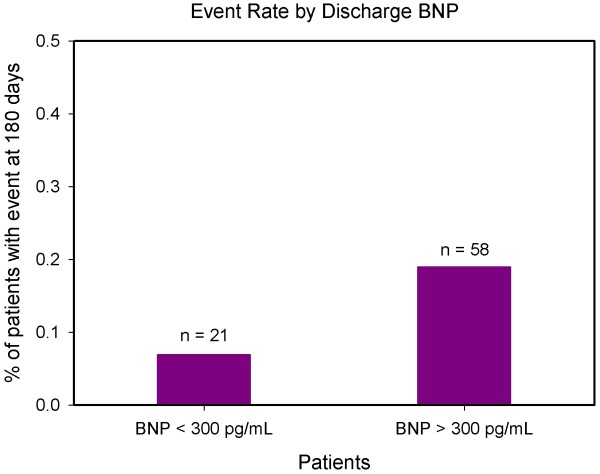
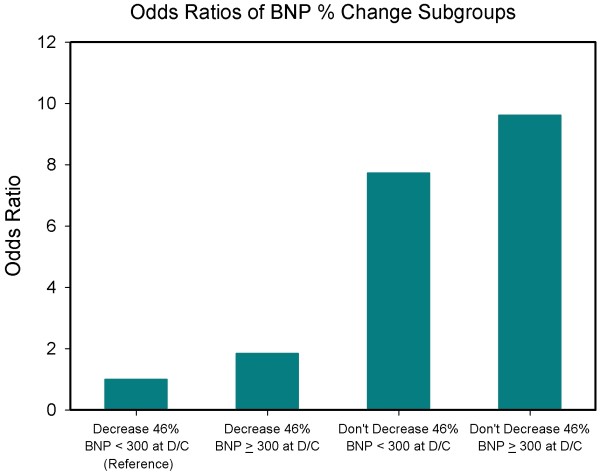
Results: BNP median (interquartile range (IQR)) value at admission was 822 (412 - 1390) pg\mL; at 24 hours was 593 (270 - 1953) and at discharge was 325 (160 - 725). A BNP reduction of >46% at discharge had an area under curve (AUC) of 0.70 (P < 0.001) for predicting future adverse events. There were 78 events through follow up and in 58 of these patients the BNP level at discharge was >300 pg/mL. A BNP reduction of 25.9% after 24 hours had an AUC at ROC curve of 0.64 for predicting adverse events (P < 0.001). The odds ratio of the patients whose BNP level at discharge was <300 pg/mL and whose percentage decrease at discharge was <46% compared to the group whose BNP level at discharge was <300 pg/mL and whose percentage decrease at discharge was >46% was 4.775 (95% confidence interval (CI) 1.76 - 12.83, P < 0.002). The odds ratio of the patients whose BNP level at discharge was >300 pg/mL and whose percentage decrease at discharge was <46% compared to the group whose BNP level at discharge was <300 pg/mL and whose percentage decrease at discharge was >46% was 9.614 (CI 4.51 - 20.47, P < 0.001).
Conclusions: A reduction of BNP >46% at hospital discharge compared to the admission levels coupled with a BNP absolute value < 300 pg/mL seems to be a very powerful negative prognostic value for future cardiovascular outcomes in patients hospitalized with ADHF.
Figures
Comment in
-
The interpretation of brain natriuretic peptide in critical care patients; will it ever be useful?Crit Care. 2010;14(4):184. doi: 10.1186/cc9083. Epub 2010 Aug 6. Crit Care. 2010. PMID: 20712913 Free PMC article.
Similar articles
-
Predictive value for death and rehospitalization of 30-day postdischarge B-type natriuretic peptide (BNP) in elderly patients with heart failure. Sub-analysis of Italian RED Study.Clin Chem Lab Med. 2015 Feb;53(3):507-13. doi: 10.1515/cclm-2013-0927. Clin Chem Lab Med. 2015. PMID: 25252752
-
The utilization and prognostic impact of B-type Natriuretic Peptide in hospitalized acute decompensated heart failure in an Asian population.BMC Cardiovasc Disord. 2016 Sep 9;16(1):178. doi: 10.1186/s12872-016-0342-z. BMC Cardiovasc Disord. 2016. PMID: 27613439 Free PMC article.
-
Prognostic Impact of BNP Variations in Patients Admitted for Acute Decompensated Heart Failure with In-Hospital Worsening Renal Function.Heart Lung Circ. 2017 Mar;26(3):226-234. doi: 10.1016/j.hlc.2016.06.1205. Epub 2016 Jul 19. Heart Lung Circ. 2017. PMID: 27523462 Clinical Trial.
-
Effectiveness of serial increases in amino-terminal pro-B-type natriuretic peptide levels to indicate the need for mechanical circulatory support in children with acute decompensated heart failure.Am J Cardiol. 2011 Feb 15;107(4):573-8. doi: 10.1016/j.amjcard.2010.10.015. Am J Cardiol. 2011. PMID: 21295174 Review.
-
Natriuretic peptide testing for predicting adverse events following heart failure hospitalization.Congest Heart Fail. 2012 Sep-Oct;18 Suppl 1:S9-S13. doi: 10.1111/j.1751-7133.2012.00306.x. Congest Heart Fail. 2012. PMID: 22891803 Review.
Cited by
-
Rise in BNP despite appropriate acute decompensated heart failure treatment : Patient characteristics and outcomes.Herz. 2017 Jun;42(4):411-417. doi: 10.1007/s00059-016-4478-5. Epub 2016 Sep 13. Herz. 2017. PMID: 27624713 Clinical Trial. English.
-
Cardiorenal biomarkers in acute heart failure.J Geriatr Cardiol. 2012 Sep;9(3):292-304. doi: 10.3724/SP.J.1263.2012.02291. J Geriatr Cardiol. 2012. PMID: 23097660 Free PMC article.
-
Serial Measurement of Amino-Terminal Pro-B-Type Natriuretic Peptide Predicts Adverse Cardiovascular Outcome in Children With Primary Myocardial Dysfunction and Acute Decompensated Heart Failure.Pediatr Crit Care Med. 2015 Jul;16(6):529-34. doi: 10.1097/PCC.0000000000000408. Pediatr Crit Care Med. 2015. PMID: 25856472 Free PMC article.
-
BNP and NT-proBNP as prognostic markers in persons with acute decompensated heart failure: a systematic review.Heart Fail Rev. 2014 Aug;19(4):453-70. doi: 10.1007/s10741-014-9442-y. Heart Fail Rev. 2014. PMID: 25062653
-
The interpretation of brain natriuretic peptide in critical care patients; will it ever be useful?Crit Care. 2010;14(4):184. doi: 10.1186/cc9083. Epub 2010 Aug 6. Crit Care. 2010. PMID: 20712913 Free PMC article.
References
-
- Cleland JG, Svedberg K, Follath F, Komajda M, Cohen-Solal A, Aguilar JC, Dietz R, Gavazzi A, Hobbs R, Korewicki J, Madeira HC, Moiseyev VS, Preda I, van Gilst WH, Widimsky J, Freemantle N, Eastaugh J, Mason J. The Euro Heart Failure survey program-a survey on the quality of care among patients with heart failure in Europe. Part 1. patient characteristics and diagnosis. Eur Heart J. 2003;24:442–463. doi: 10.1016/S0195-668X(02)00823-0. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
