

Alternative management of diabetic ketoacidosis in a Brazilian pediatric emergency department
- PMID: 20550713
- PMCID: PMC2903515
- DOI: 10.1186/1758-5996-2-41
Alternative management of diabetic ketoacidosis in a Brazilian pediatric emergency department
Abstract
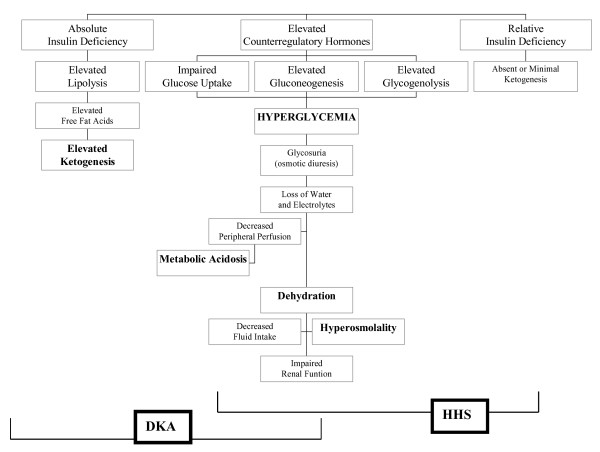
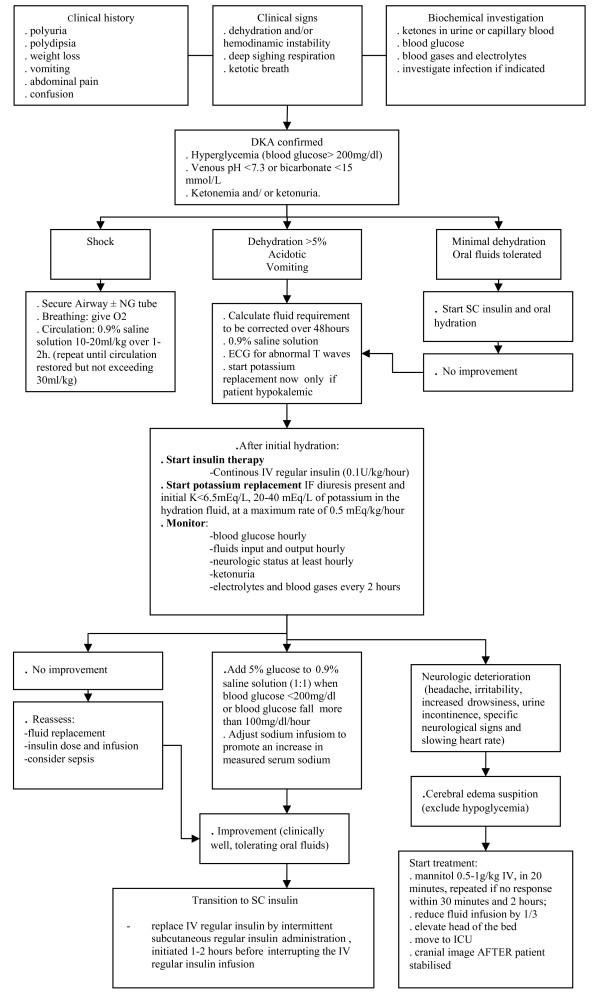
DKA is a severe metabolic derangement characterized by dehydration, loss of electrolytes, hyperglycemia, hyperketonemia, acidosis and progressive loss of consciousness that results from severe insulin deficiency combined with the effects of increased levels of counterregulatory hormones (catecholamines, glucagon, cortisol, growth hormone). The biochemical criteria for diagnosis are: blood glucose > 200 mg/dl, venous pH <7.3 or bicarbonate <15 mEq/L, ketonemia >3 mmol/L and presence of ketonuria. A patient with DKA must be managed in an emergency ward by an experienced staff or in an intensive care unit (ICU), in order to provide an intensive monitoring of the vital and neurological signs, and of the patient's clinical and biochemical response to treatment. DKA treatment guidelines include: restoration of circulating volume and electrolyte replacement; correction of insulin deficiency aiming at the resolution of metabolic acidosis and ketosis; reduction of risk of cerebral edema; avoidance of other complications of therapy (hypoglycemia, hypokalemia, hyperkalemia, hyperchloremic acidosis); identification and treatment of precipitating events. In Brazil, there are few pediatric ICU beds in public hospitals, so an alternative protocol was designed to abbreviate the time on intravenous infusion lines in order to facilitate DKA management in general emergency wards. The main differences between this protocol and the international guidelines are: intravenous fluid will be stopped when oral fluids are well tolerated and total deficit will be replaced orally; if potassium analysis still indicate need for replacement, it will be given orally; subcutaneous rapid-acting insulin analog is administered at 0.15 U/kg dose every 2-3 hours until resolution of metabolic acidosis; approximately 12 hours after treatment initiation, intermediate-acting (NPH) insulin is initiated at the dose of 0.6-1 U/kg/day, and it will be lowered to 0.4-0.7 U/kg/day at discharge from hospital.
Figures
Similar articles
-
Treatment Challenges and Controversies in the Management of Critically Ill Diabetic Ketoacidosis (DKA) Patients in Intensive Care Units.Cureus. 2024 Sep 6;16(9):e68785. doi: 10.7759/cureus.68785. eCollection 2024 Sep. Cureus. 2024. PMID: 39360087 Free PMC article. Review.
-
The Effects of Subcutaneous Rapid-Acting Insulin Aspart in the Treatment of Mild and Moderate Diabetic Ketoacidosis in Children: A Prospective Study.Cureus. 2024 Jul 10;16(7):e64241. doi: 10.7759/cureus.64241. eCollection 2024 Jul. Cureus. 2024. PMID: 39130949 Free PMC article.
-
Euglycemic diabetic ketoacidosis: A missed diagnosis.World J Diabetes. 2021 May 15;12(5):514-523. doi: 10.4239/wjd.v12.i5.514. World J Diabetes. 2021. PMID: 33995841 Free PMC article. Review.
-
Current concepts of the pathogenesis and management of diabetic ketoacidosis (DKA).Ann Acad Med Singap. 1983 Oct;12(4):596-605. Ann Acad Med Singap. 1983. PMID: 6331271 Review.
-
Management of decompensated diabetes. Diabetic ketoacidosis and hyperglycemic hyperosmolar syndrome.Crit Care Clin. 2001 Jan;17(1):75-106. doi: 10.1016/s0749-0704(05)70153-6. Crit Care Clin. 2001. PMID: 11219236 Review.
Cited by
-
Managing diabetic ketoacidosis in non-intensive care unit setting: Role of insulin analogs.Indian J Pharmacol. 2011 Jul;43(4):398-401. doi: 10.4103/0253-7613.83109. Indian J Pharmacol. 2011. PMID: 21844993 Free PMC article.
-
Misleading Presentation of Euglycemic Diabetic Ketoacidosis: Implication for Low-Mid-Income Communities.N Am J Med Sci. 2015 Nov;7(11):537-9. doi: 10.4103/1947-2714.170629. N Am J Med Sci. 2015. PMID: 26713304 Free PMC article. No abstract available.
-
Comparison of subcutaneous insulin aspart and intravenous regular insulin for the treatment of mild and moderate diabetic ketoacidosis in pediatric patients.Endocrine. 2018 Aug;61(2):267-274. doi: 10.1007/s12020-018-1635-z. Epub 2018 May 24. Endocrine. 2018. PMID: 29797212 Clinical Trial.
-
Frequency and associated risk factors of recurrent diabetic ketoacidosis among Saudi adolescents with type 1 diabetes mellitus.Saudi Med J. 2015 Feb;36(2):216-20. doi: 10.15537/smj.2015.2.10560. Saudi Med J. 2015. PMID: 25719588 Free PMC article.
-
Subcutaneous rapid-acting insulin analogues for diabetic ketoacidosis.Cochrane Database Syst Rev. 2016 Jan 21;2016(1):CD011281. doi: 10.1002/14651858.CD011281.pub2. Cochrane Database Syst Rev. 2016. PMID: 26798030 Free PMC article.
References
-
- Rewers A, Klingensmith G, Davis C, Petitti DB, Pihoker C, Rodriguez B, Schwartz D, Imperatore G, Williams D, Dolan LM, Dabelea D. Diabetic ketoacidosis at onset of diabetes: the SEARCH for diabetes in youth study. Diabetes. 2005;54(suppl 1):A63. - PubMed
-
- Rodacki M, Pereira JR, Nabuco de Oliveira AM, Barone B, Mac Dowell R, Perricelli P, Bravo MT, de Oliveira MM, Brum JD, Belem LC, de Ornellas PG, Berardo RS, Luescher J, Campos L, Vangelotti Ade M, Kupfer R, Zajdenverg L, Milech A, Paulo de Oliveira. Ethnicity and young age influence the frequency of diabetic ketoacidosis at the onset of type 1 diabetes. Diabetes Res Clin Pract. 2007;78(2):259–62. doi: 10.1016/j.diabres.2007.04.002. - DOI - PubMed
-
- Barone B, Rodacki M, Cenci MC, Zajdenverg L, Milech A, Oliveira JE. Diabetic ketoacidosis in adults--update of an old complication. Arq Bras Endocrinol Metabol. 2007;51(9):1434–47. - PubMed
LinkOut - more resources
Full Text Sources
