

Rectoanal reflexes and sensorimotor response in rectal hyposensitivity
- PMID: 20551758
- PMCID: PMC3929945
- DOI: 10.1007/DCR.0b013e3181dcb2d6
Rectoanal reflexes and sensorimotor response in rectal hyposensitivity
Abstract
Purpose: Rectal hyposensitivity commonly causes anorectal disorders, but its underlying mechanism is unknown. We hypothesized that subjects with rectal hyposensitivity have altered rectoanal reflexes and/or sensorimotor response.
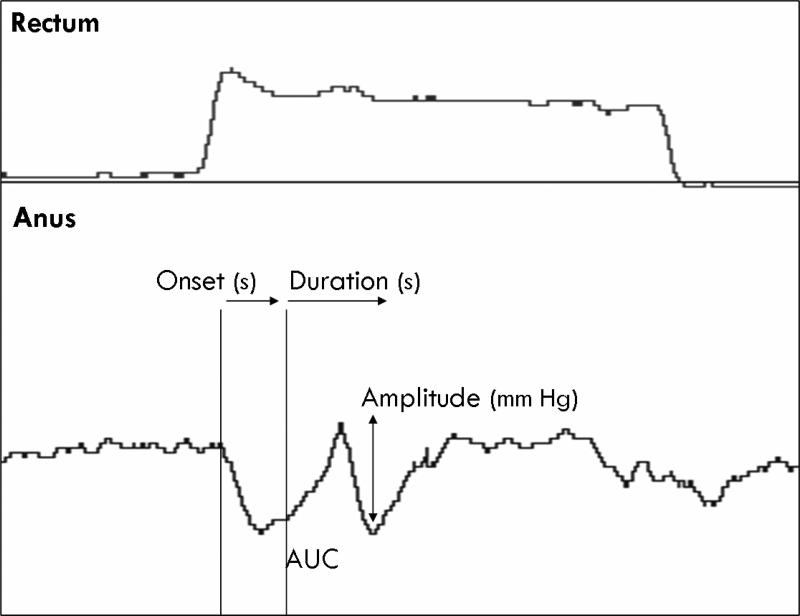
Methods: We performed stepwise graded balloon distensions of the rectum in 30 subjects with constipation and rectal hyposensitivity and in 23 healthy controls. Thresholds for first sensation, desire, and urgency to defecate were assessed. The lowest balloon volume that evoked rectoanal inhibitory reflex, rectoanal contractile reflex, and sensorimotor response and manometric characteristics and rectal compliance were examined.
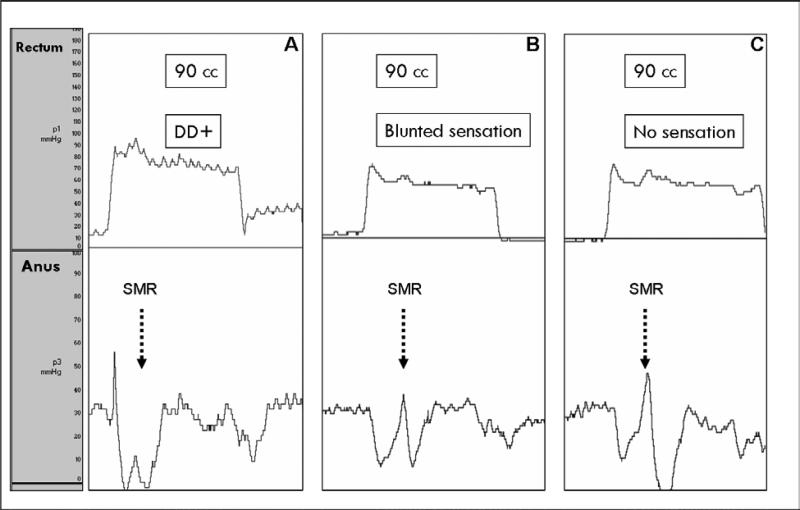
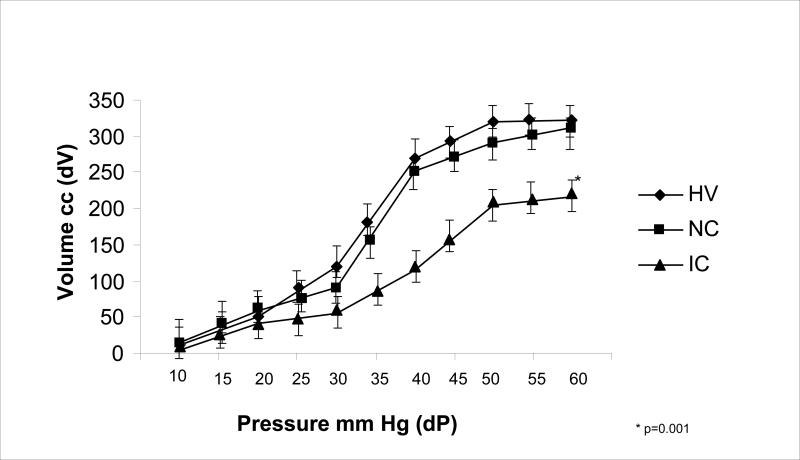
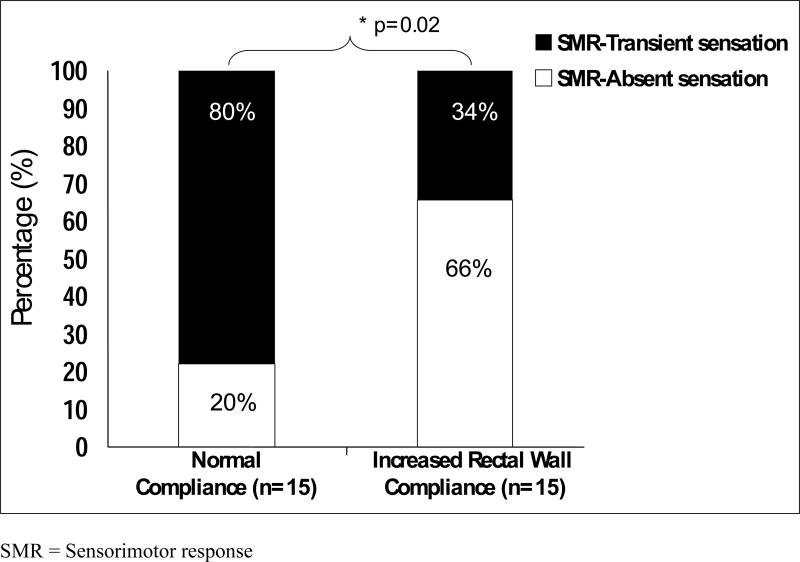
Results: Reflex responses were present in all subjects. The balloon volumes were higher in subjects with rectal hyposensitivity for inducing rectoanal inhibitory reflex (P = .008) and contractile reflex (P = .001) compared with controls. All controls showed a sensorimotor response, but in 13 hyposensitive subjects (43%) the onset of sensorimotor response was associated with absent sensation and in 17 (57%), with a transient rectal sensation. Thresholds for eliciting sensorimotor response were similar between patients and controls, but the amplitude, duration, and magnitude of response were higher (P < .05) in patients. Rectal compliance was similar between controls and hyposensitive subjects with transient sensation but higher (P = .001) in subjects with absent sensation.
Conclusions: Constipated subjects with rectal hyposensitivity demonstrate higher thresholds for inducing rectoanal reflexes and abnormal characteristics of sensorimotor response. These findings suggest either disruption of afferent gut-brain pathways or rectal wall dysfunction. These altered features may play a role in the pathogenesis of bowel dysfunction in rectal hyposensitivity.
Figures

References
-
- Rogers J. Anal and rectal sensation. Baillieres Clin Gastroenterol. 1992;6:179–91. - PubMed
-
- Gladman MA, Lunniss PJ, Scott SM, Swash M. Rectal hyposensitivity. Am J Gastroenterol. 2006;101:1140–1151. - PubMed
-
- Gladman MA, Dvorkin LS, Lunniss PJ, Williams NS, Scott SM. Rectal hyposensitivity: a disorder of the rectal wall or the afferent pathway? An assessment using the barostat. Am J Gastroenterol. 2005;100:106–114. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
