

DNA vaccine encoding prostatic acid phosphatase (PAP) elicits long-term T-cell responses in patients with recurrent prostate cancer
- PMID: 20551832
- PMCID: PMC3045767
- DOI: 10.1097/CJI.0b013e3181dda23e
DNA vaccine encoding prostatic acid phosphatase (PAP) elicits long-term T-cell responses in patients with recurrent prostate cancer
Abstract
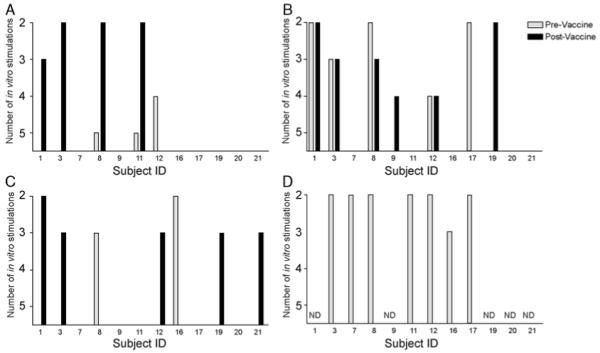
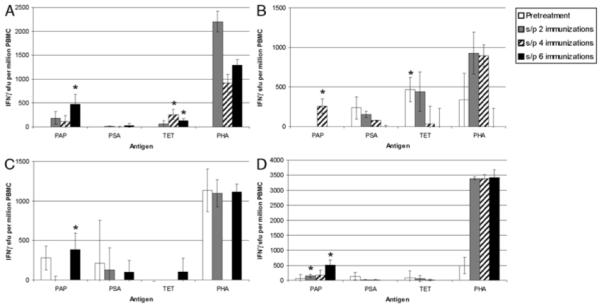
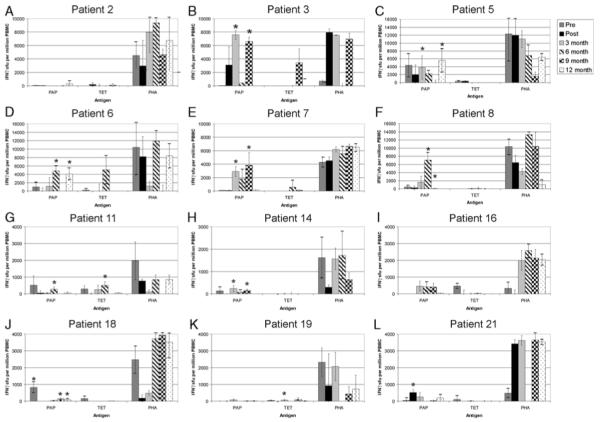
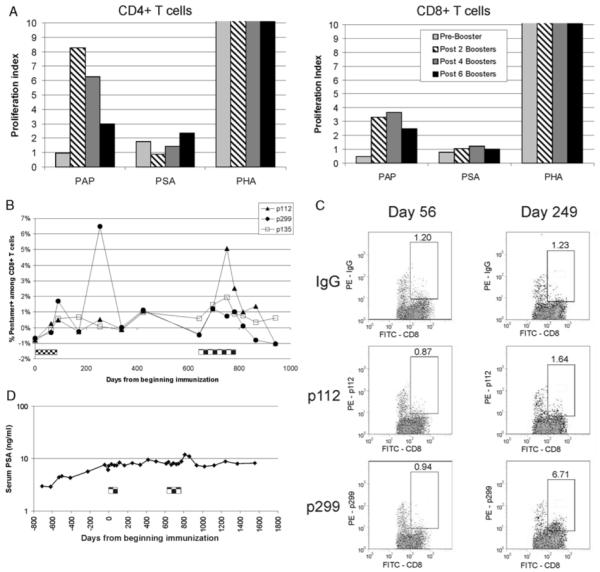
Prostatic acid phosphatase (PAP) is a tumor antigen in prostate cancer and the target of several anti-tumor vaccines in earlier clinical trials. Ultimately, the goal of anti-tumor vaccines is to elicit a sustainable immune response, able to eradicate a tumor, or at least restrain its growth. We have investigated plasmid DNA vaccines and have previously conducted a phase 1 trial in which patients with recurrent prostate cancer were vaccinated with a DNA vaccine encoding PAP. In this study, we investigated the immunologic efficacy of subsequent booster immunizations, and conducted more detailed longitudinal immune analysis, to answer several questions aimed at guiding optimal schedules of vaccine administration for future clinical trials. We report that antigen-specific cytolytic T-cell responses were amplified after immunization in 7 of 12 human leukocyte antigen-A2-expressing individuals, and that multiple immunizations seemed necessary to elicit PAP-specific interferon-gamma-secreting immune responses detectable by enzyme-linked immunosorbent spot assay. Moreover, among individuals who experienced a >/=200% increase in prostate-specific antigen doubling time, long-term PAP-specific interferon-gamma-secreting T-cell responses were detectable in 6 of 8, but in only 1 of 14 individuals without an observed change in prostate-specific antigen doubling time (P=0.001). Finally, we identified that immune responses elicited could be further amplified by subsequent booster immunizations. These results suggest that future trials using this DNA vaccine, and potentially other anti-tumor DNA vaccines, could investigate ongoing schedules of administration with periodic booster immunizations. Moreover, these results suggest that DNA vaccines targeting PAP could potentially be combined in heterologous immunization strategies with other vaccines to further augment PAP-specific T-cell immunity.
Figures
Similar articles
-
HLA-A2-restricted T-cell epitopes specific for prostatic acid phosphatase.Cancer Immunol Immunother. 2010 Jun;59(6):943-53. doi: 10.1007/s00262-010-0820-6. Epub 2010 Feb 6. Cancer Immunol Immunother. 2010. PMID: 20140431 Free PMC article.
-
Plasmid DNA vaccine encoding prostatic acid phosphatase is effective in eliciting autologous antigen-specific CD8+ T cells.Cancer Immunol Immunother. 2007 Jun;56(6):885-95. doi: 10.1007/s00262-006-0241-8. Epub 2006 Nov 11. Cancer Immunol Immunother. 2007. PMID: 17102977 Free PMC article.
-
Safety and immunological efficacy of a DNA vaccine encoding prostatic acid phosphatase in patients with stage D0 prostate cancer.J Clin Oncol. 2009 Sep 1;27(25):4047-54. doi: 10.1200/JCO.2008.19.9968. Epub 2009 Jul 27. J Clin Oncol. 2009. PMID: 19636017 Free PMC article. Clinical Trial.
-
Dendritic cell gene therapy.Surg Oncol Clin N Am. 2002 Jul;11(3):645-60. doi: 10.1016/s1055-3207(02)00027-3. Surg Oncol Clin N Am. 2002. PMID: 12487060 Review.
-
Antigen-specific vaccines for cancer treatment.Hum Vaccin Immunother. 2014;10(11):3332-46. doi: 10.4161/21645515.2014.973317. Hum Vaccin Immunother. 2014. PMID: 25483639 Free PMC article. Review.
Cited by
-
FLT PET/CT imaging of metastatic prostate cancer patients treated with pTVG-HP DNA vaccine and pembrolizumab.J Immunother Cancer. 2019 Jan 30;7(1):23. doi: 10.1186/s40425-019-0516-1. J Immunother Cancer. 2019. PMID: 30700328 Free PMC article. Clinical Trial.
-
Immunotherapy for prostate cancer: recent developments and future challenges.Cancer Metastasis Rev. 2014 Sep;33(2-3):641-55. doi: 10.1007/s10555-013-9479-8. Cancer Metastasis Rev. 2014. PMID: 24477411 Free PMC article. Review.
-
Real-time immune monitoring to guide plasmid DNA vaccination schedule targeting prostatic acid phosphatase in patients with castration-resistant prostate cancer.Clin Cancer Res. 2014 Jul 15;20(14):3692-704. doi: 10.1158/1078-0432.CCR-14-0169. Epub 2014 May 21. Clin Cancer Res. 2014. PMID: 24850844 Free PMC article.
-
Safety and immunogenicity of novel 5T4 viral vectored vaccination regimens in early stage prostate cancer: a phase I clinical trial.J Immunother Cancer. 2020 Jun;8(1):e000928. doi: 10.1136/jitc-2020-000928. J Immunother Cancer. 2020. PMID: 32591433 Free PMC article. Clinical Trial.
-
Trial watch: Naked and vectored DNA-based anticancer vaccines.Oncoimmunology. 2015 Apr 2;4(5):e1026531. doi: 10.1080/2162402X.2015.1026531. eCollection 2015 May. Oncoimmunology. 2015. PMID: 26155408 Free PMC article.
References
-
- Meidenbauer N, Harris DT, Spitler LE, et al. Generation of PSA-reactive effector cells after vaccination with a PSA-based vaccine in patients with prostate cancer. Prostate. 2000;43:88–100. - PubMed
-
- Eder JP, Kantoff PW, Roper K, et al. A phase I trial of a recombinant vaccinia virus expressing prostate-specific antigen in advanced prostate cancer. Clin Cancer Res. 2000;6:1632–1638. - PubMed
-
- Gulley J, Chen AP, Dahut W, et al. Phase I study of a vaccine using recombinant vaccinia virus expressing PSA (rV-PSA) in patients with metastatic androgen-independent prostate cancer. Prostate. 2002;53:109–117. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
