

Long-term survival and recurrence outcomes following surgery for distal rectal cancer
- PMID: 20552409
- PMCID: PMC3071558
- DOI: 10.1245/s10434-010-1119-8
Long-term survival and recurrence outcomes following surgery for distal rectal cancer
Abstract
Background: Treatment of distal rectal cancer remains clinically challenging and includes proctectomy and coloanal anastomosis (CAA) or abdominoperineal resection (APR). The purpose of this study is to evaluate operative and pathologic factors associated with long-term survival and local recurrence outcomes in patients treated for distal rectal cancer.
Methods: A retrospective consecutive cohort study of 304 patients treated for distal rectal cancer with radical resection from 1993 to 2003 was performed. Patients were grouped by procedure (CAA or APR). Demographic, pathologic, recurrence, and survival data were analyzed utilizing chi-square analysis for comparison of proportions. Survival analysis was performed using Kaplan-Meier method and log-rank test for univariate and Cox regression for multivariate comparison.
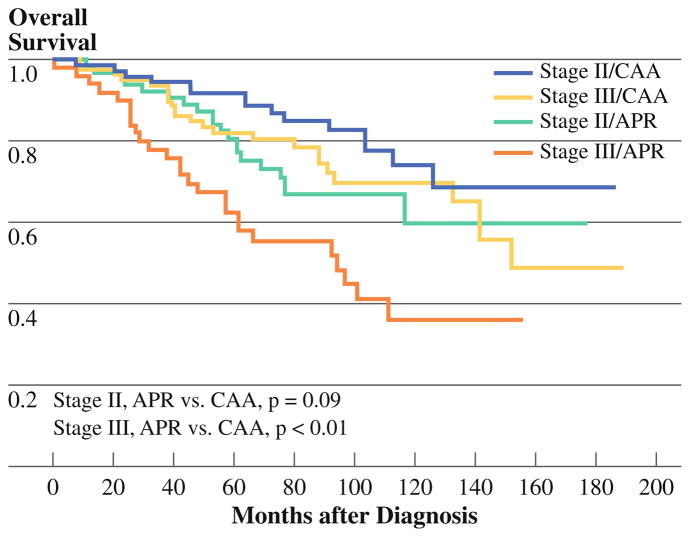
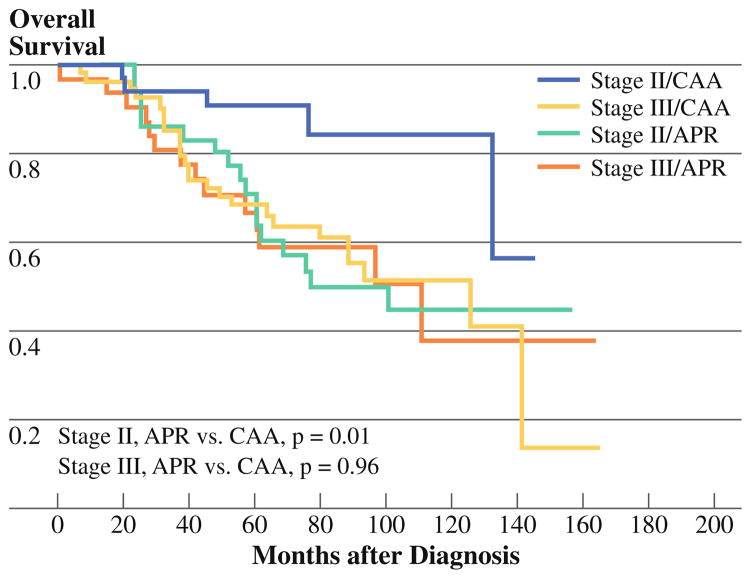
Results: The median tumor distance from the anal verge was 2 cm [interquartile range (IQR) 0.5-4 cm]. Margins were negative in all but four patients (one distal, 0.3%; three radial, 1%). The 5-year overall survival rate was 82% (88.6% stage pI, 80.5% stage pII, 67.9% stage pIII). Older age, advanced pathologic stage, presence of lymphovascular or perineural invasion, earlier treatment period, and APR surgery type were associated with worse survival on multivariate analysis. The 5-year local recurrence rate was 5.3% after CAA and 7.9% after APR (p = 0.33).
Conclusions: Low rates of local recurrence and good overall survival can be achieved after treatment of distal rectal cancer with stage-appropriate chemoradiation and proctectomy with CAA or APR. Sphincter preservation can be achieved even with distal margins less than 2 cm.
Figures
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2009. CA Cancer J Clin. 2009 doi: 10.3322/caac.200006. - DOI
-
- NIH Consensus Conference. Adjuvant therapy for patients with colon and rectal cancer. JAMA. 1990;264:1444–50. - PubMed
-
- Sauer R, Becker H, Hohenberger W, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. New Engl J Med. 2004;351:1731–40. - PubMed
-
- Kapiteijn E, Marijnen C, Negtegaal ID, et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N Engl J Med. 2001;345:638–46. - PubMed
-
- Law WL, Chu KW. Abdominoperineal resection is associated with poor oncologic outcome. Br J Surg. 2004;91:1493–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
