

Recurrent respiratory papillomatosis: a complex defect in immune responsiveness to human papillomavirus-6 and -11
- PMID: 20553528
- PMCID: PMC2909665
- DOI: 10.1111/j.1600-0463.2010.02617.x
Recurrent respiratory papillomatosis: a complex defect in immune responsiveness to human papillomavirus-6 and -11
Abstract
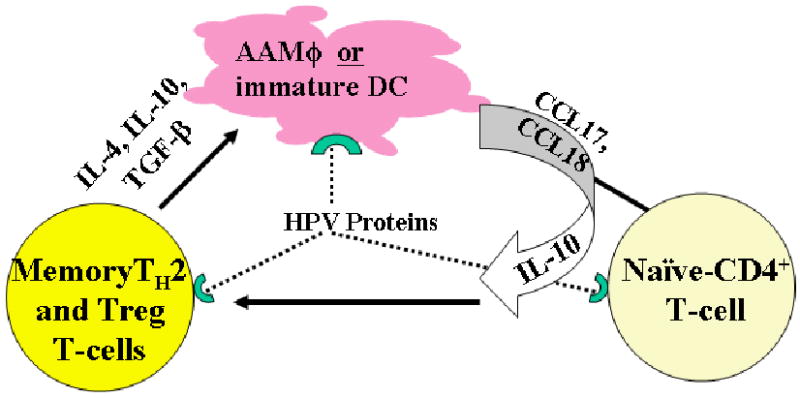
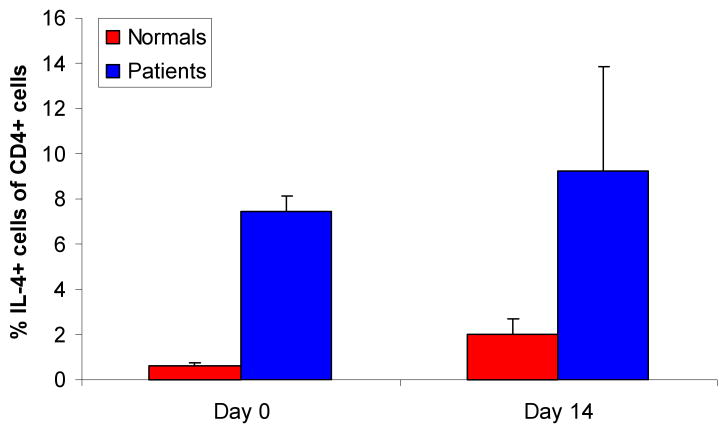
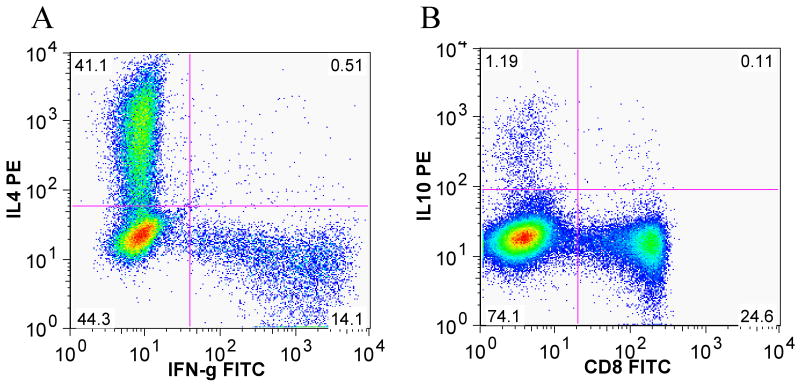
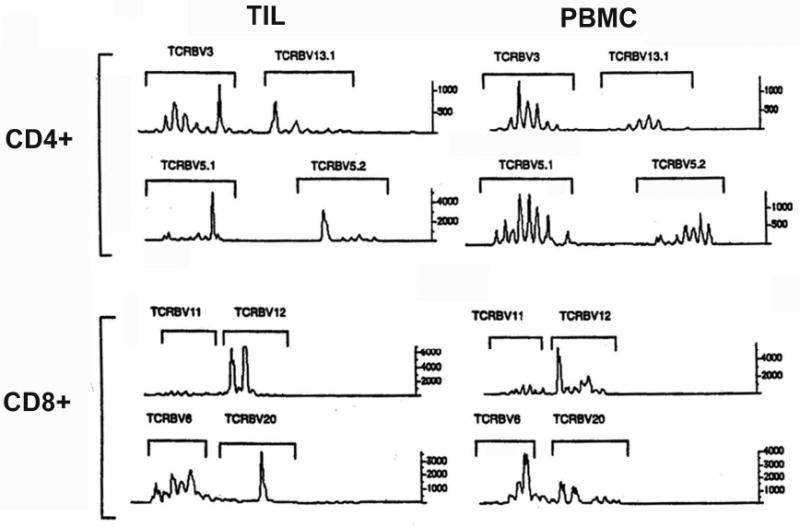
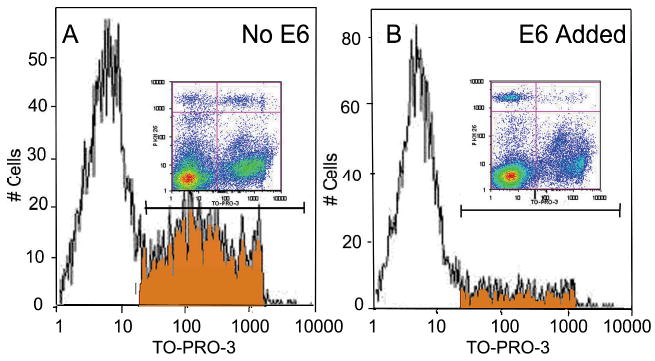
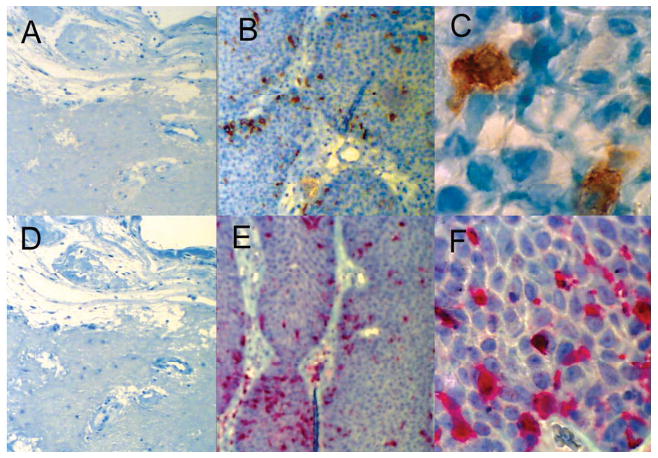
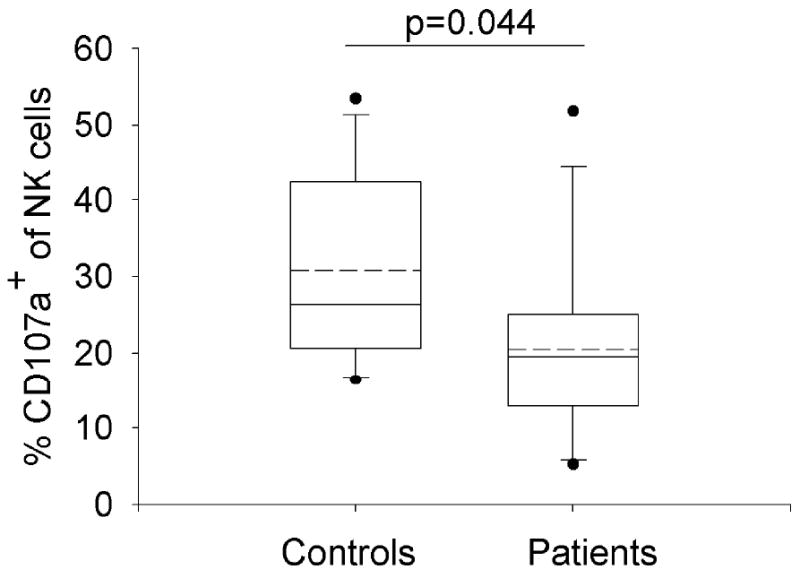
Recurrent respiratory papillomatosis (RRP) is a rare disease of the larynx caused by infection with human papillomaviruses (HPV) -6 or -11, associated with significant morbidity and on occasion mortality. Here we summarize our current understanding of the permissive adaptive and innate responses made by patients with RRP that support chronic HPV infection and prevent immune clearance of these viruses. Furthermore, we provide new evidence of T(H)2-like polarization in papillomas and blood of patients with RRP, restricted CD4 and CD8 Vbeta repertoires, the effect of HPV-11 early protein E6 on T-cell alloreactivity, enriched Langerhans cell presence in papillomas, and evidence that natural killer cells are dysfunctional in RRP. We review the immunogenetic mechanisms that regulate the dysfunctional responses made by patients with RRP in response to HPV infection of the upper airway. In addition, we are identifying T-cell epitopes on HPV-11 early proteins, in the context of human leukocyte antigen (HLA) class II alleles enriched in RRP that should help generate a therapeutic vaccine. Taken together, RRP is a complex, multigene disease manifesting as a tissue and HPV-specific, immune deficiency that prevents effective clearance and/or control of HPV-6 and -11 infection.
Figures
References
-
- Holinger PH, Johnson KC, Anison GC. Papilloma of larynx: review of 109 cases with preliminary report of aureomycin therapy. Ann Otol Rhinol Laryngol. 1950;59:547–563. - PubMed
-
- Armstrong LR, Preston EJ, Reichert M, et al. Incidence and prevalence of recurrent respiratory papillomatosis among children in Atlanta and Seattle. Clin Infect Dis. 2000;31:107–109. - PubMed
-
- Broker TR, Jin G, Croom-Rivers A, et al. Dev Biol (Basel) Vol. 106. 2001. Viral latency--the papillomavirus model; pp. 443–451. discussion 452-443, 465-475. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
