

Intraoperative fluid optimization using stroke volume variation in high risk surgical patients: results of prospective randomized study
- PMID: 20553586
- PMCID: PMC2911766
- DOI: 10.1186/cc9070
Intraoperative fluid optimization using stroke volume variation in high risk surgical patients: results of prospective randomized study
Abstract
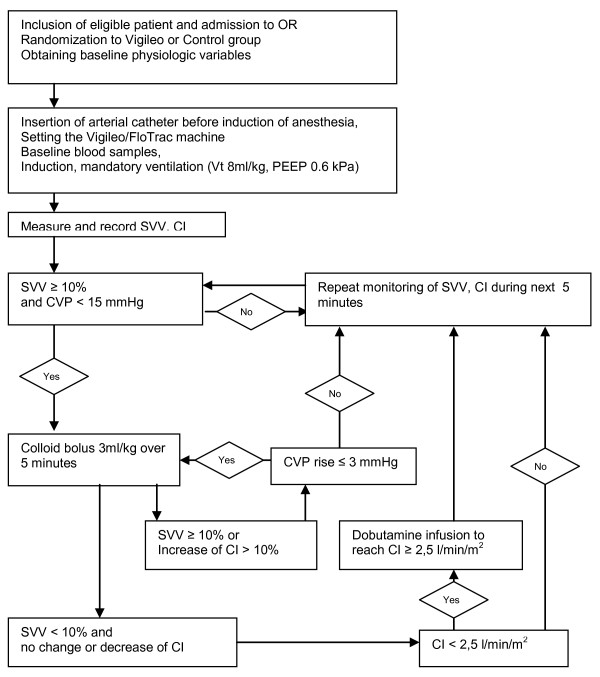
Introduction: Stroke volume variation (SVV) is a good and easily obtainable predictor of fluid responsiveness, which can be used to guide fluid therapy in mechanically ventilated patients. During major abdominal surgery, inappropriate fluid management may result in occult organ hypoperfusion or fluid overload in patients with compromised cardiovascular reserves and thus increase postoperative morbidity. The aim of our study was to evaluate the influence of SVV guided fluid optimization on organ functions and postoperative morbidity in high risk patients undergoing major abdominal surgery.
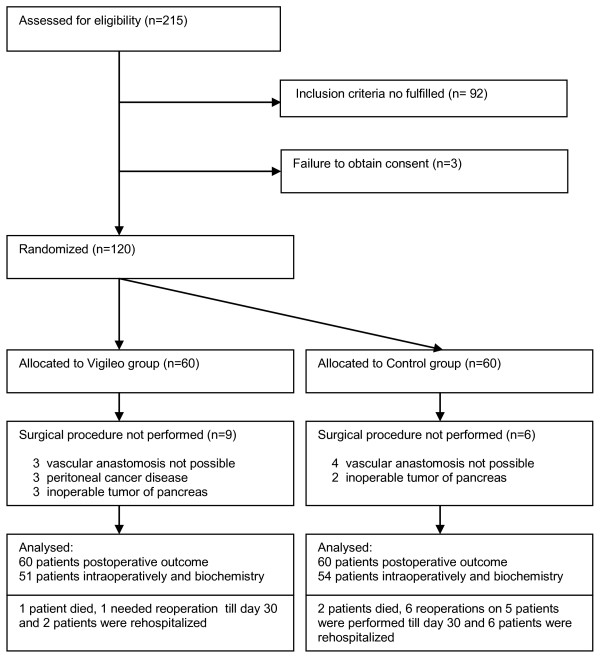
Methods: Patients undergoing elective intraabdominal surgery were randomly assigned to a Control group (n = 60) with routine intraoperative care and a Vigileo group (n = 60), where fluid management was guided by SVV (Vigileo/FloTrac system). The aim was to maintain the SVV below 10% using colloid boluses of 3 ml/kg. The laboratory parameters of organ hypoperfusion in perioperative period, the number of infectious and organ complications on day 30 after the operation, and the hospital and ICU length of stay and mortality were evaluated. The local ethics committee approved the study.
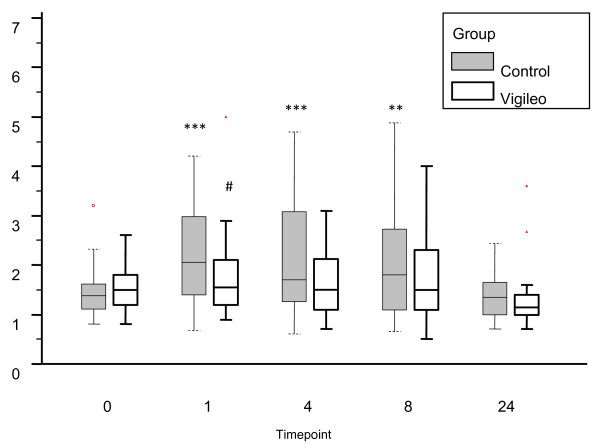
Results: The patients in the Vigileo group received more colloid (1425 ml [1000-1500] vs. 1000 ml [540-1250]; P = 0.0028) intraoperatively and a lower number of hypotensive events were observed (2[1-2] Vigileo vs. 3.5[2-6] in Control; P = 0.0001). Lactate levels at the end of surgery were lower in Vigileo (1.78 +/- 0.83 mmol/l vs. 2.25 +/- 1.12 mmol/l; P = 0.0252). Fewer Vigileo patients developed complications (18 (30%) vs. 35 (58.3%) patients; P = 0.0033) and the overall number of complications was also reduced (34 vs. 77 complications in Vigileo and Control respectively; P = 0.0066). A difference in hospital length of stay was found only in per protocol analysis of patients receiving optimization (9 [8-12] vs. 10 [8-19] days; P = 0.0421). No difference in mortality (1 (1.7%) vs. 2 (3.3%); P = 1.0) and ICU length of stay (3 [2-5] vs. 3 [0.5-5]; P = 0.789) was found.
Conclusions: In this study, fluid optimization guided by SVV during major abdominal surgery is associated with better intraoperative hemodynamic stability, decrease in serum lactate at the end of surgery and lower incidence of postoperative organ complications.
Trial registration: Current Controlled Trials ISRCTN95085011.
Figures
Comment in
-
Improving surgical outcomes: it is the destination not the journey.Crit Care. 2010;14(4):177. doi: 10.1186/cc9082. Epub 2010 Jul 16. Crit Care. 2010. PMID: 20670387 Free PMC article.
-
Balanced study groups in a randomized trial--authors' response.Crit Care. 2011;15(6):460. doi: 10.1186/cc10549. Epub 2011 Dec 8. Crit Care. 2011. PMID: 22189038 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
