

Using serological measures to monitor changes in malaria transmission in Vanuatu
- PMID: 20553604
- PMCID: PMC2904786
- DOI: 10.1186/1475-2875-9-169
Using serological measures to monitor changes in malaria transmission in Vanuatu
Abstract
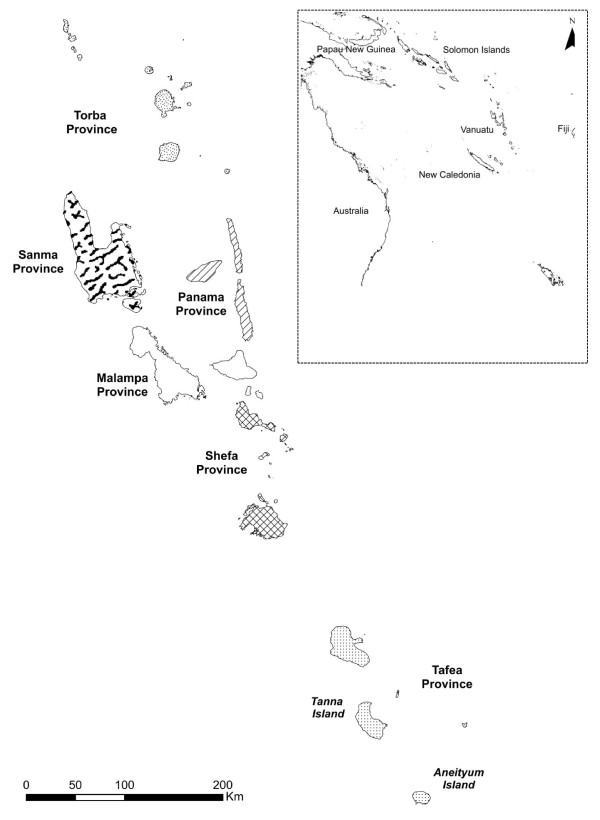
Background: With renewed interest in malaria elimination, island environments present unique opportunities to achieve this goal. However, as transmission decreases, monitoring and evaluation programmes need increasingly sensitive tools to assess Plasmodium falciparum and Plasmodium vivax exposure. In 2009, to assess the role of serological markers in evaluating malaria transmission, a cross-sectional seroprevalence study was carried out in Tanna and Aneityum, two of the southernmost islands of the Vanuatu archipelago, areas where malaria transmission has been variably reduced over the past few decades.
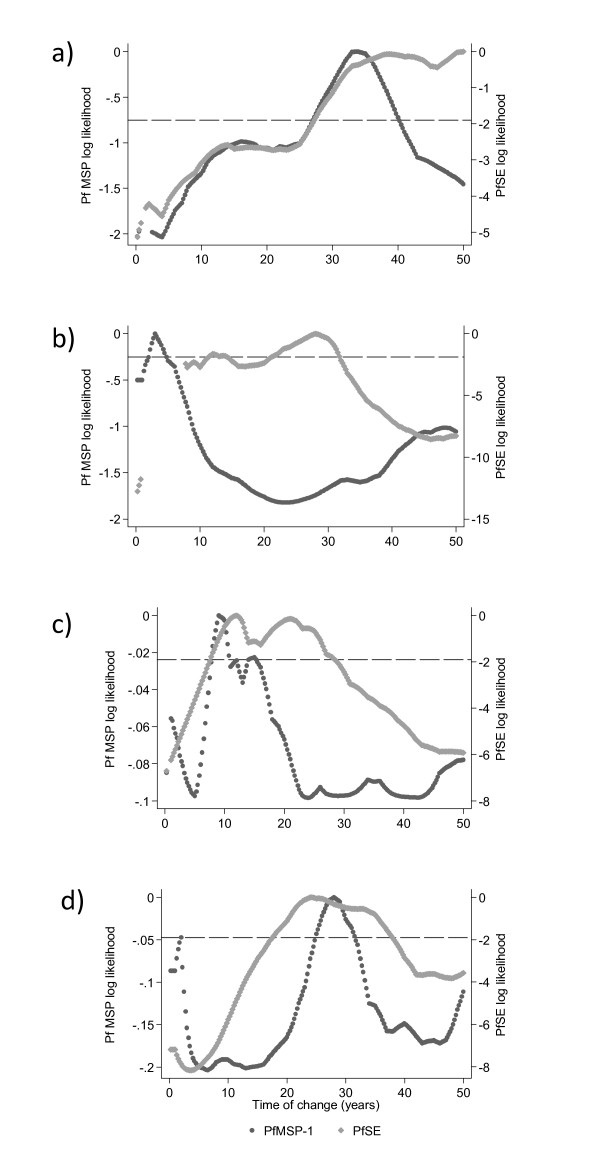
Methods: Malaria transmission was assessed using serological markers for exposure to P. falciparum and P. vivax. Filter blood spot papers were collected from 1,249 people from Tanna, and 517 people from Aneityum to assess the prevalence of antibodies to two P. falciparum antigens (MSP-119 and AMA-1) and two P. vivax antigens (MSP-119 and AMA-1). Age-specific prevalence was modelled using a simple catalytic conversion model based on maximum likelihood to generate a community seroconversion rate (SCR).
Results: Overall seropositivity in Tanna was 9.4%, 12.4% and 16.6% to P. falciparum MSP-119, AMA-1 and Schizont Extract respectively and 12.6% and 15.0% to P. vivax MSP-119 and AMA-1 respectively. Serological results distinguished between areas of differential dominance of either P. vivax or P. falciparum and analysis of age-stratified results showed a step in seroprevalence occurring approximately 30 years ago on both islands, indicative of a change in transmission intensity at this time. Results from Aneityum suggest that several children may have been exposed to malaria since the 2002 P. vivax epidemic.
Conclusion: Seroepidemiology can provide key information on malaria transmission for control programmes, when parasite rates are low. As Vanuatu moves closer to malaria elimination, monitoring changes in transmission intensity and identification of residual malaria foci is paramount in order to concentrate intervention efforts.
Figures





References
-
- Feachem RGA, Phillips AA, Targett GA. Shrinking the Malaria Map: A prospectus on Malaria Elimination. The Global Health Group; 2009.
-
- Bousema T, Drakeley C, Gesase S, Hashim R, Magesa S, Mosha F, Otieno S, Carneiro I, Cox J, Msuya E, Kleinschmidt I, Maxwell C, Greenwood B, Riley E, Sauerwein R, Chandramohan D, Gosling R. Identification of hot spots of malaria transmission for targeted malaria control. J Infect Dis. 2010;201:1764–1774. doi: 10.1086/652456. - DOI - PubMed
-
- Teklehaimanot HD, Teklehaimanot A, Kiszewski A, Rampao HS, Sachs JD. Malaria in Sao Tome and principe: on the brink of elimination after three years of effective antimalarial measures. Am J Trop Med Hyg. 2009;80:133–140. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
