

Potential diagnostic utility of intermittent administration of short-acting gonadotropin-releasing hormone agonist in gonadotropin deficiency
- PMID: 20553679
- PMCID: PMC2944005
- DOI: 10.1016/j.fertnstert.2010.04.019
Potential diagnostic utility of intermittent administration of short-acting gonadotropin-releasing hormone agonist in gonadotropin deficiency
Abstract
Objective: To determine if intermittent, low-dose, short-acting gonadotropin-releasing hormone agonist (GnRH-agonist) administration sufficiently up-regulates pituitary-gonadal function in gonadotropin deficiency to be of diagnostic or therapeutic value.
Design: Case-control study.
Setting: General clinical research center.
Patient(s): Normal adult volunteers and gonadotropin-deficiency patients.
Intervention(s): Low-dose leuprolide acetate administered subcutaneously at 4- to 5-day intervals up to 1 year.
Main outcome measure(s): Levels of luteinizing hormone (LH), follicle-stimulating hormone (FSH), and sex steroid responses.
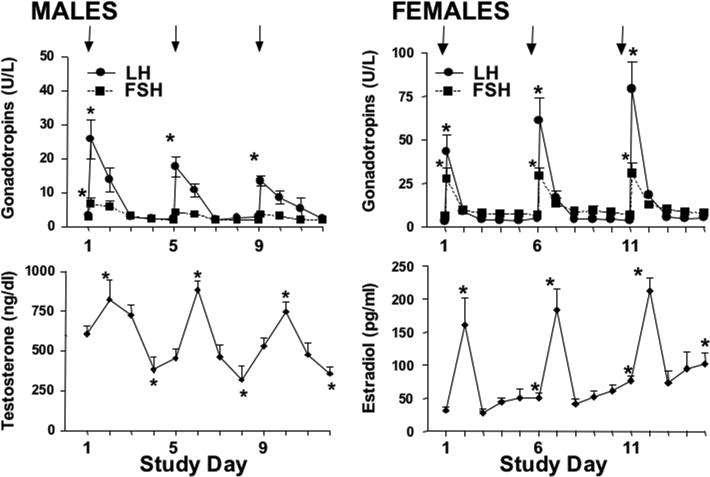
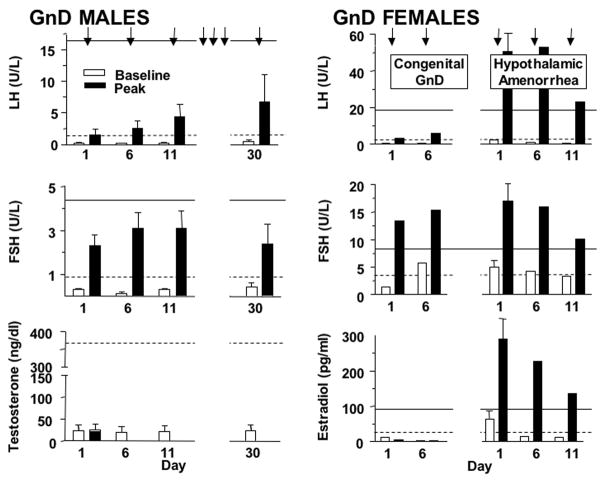
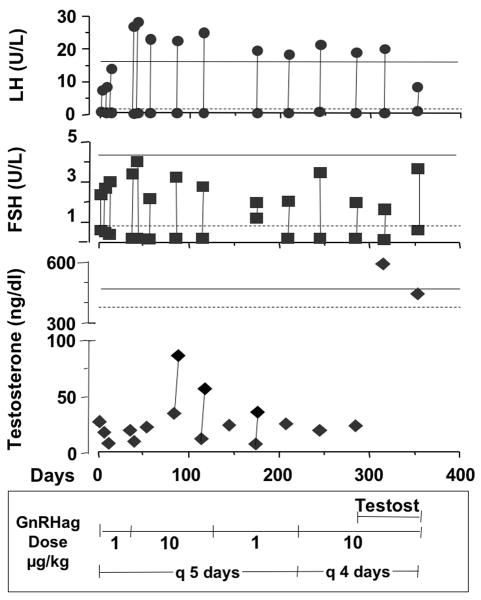
Result(s): In normal men and women, low-dose GnRH-agonist repetitively transiently stimulated gonadotropins in a gender-dimorphic manner. In congenitally gonadotropin-deficient men (n = 6) and women (n = 1), none of whom had a normal LH response to an initial GnRH-agonist test dose, this regimen consistently stimulated LH to the normal baseline range within 2 weeks. Long-term GnRH-agonist administration to a partially gonadotropin-deficient man did not alleviate hypogonadism, however. Women with hypothalamic amenorrhea (n = 2) responded normally to a single GnRH-agonist injection; however, repeated dosing did not seem to induce the normal priming effect.
Conclusion(s): The subnormal LH response to GnRH-agonist in patients with congenital gonadotropin deficiency normalized in response to repetitive intermittent GnRH-agonist administration but not sufficiently to improve hypogonadism. Hypothalamic amenorrhea patients lacked the priming response to repeated GnRH-agonist but otherwise had normal hormonal responses to GnRH-agonist. We conclude that intermittent administration of a short-acting GnRH-agonist is of potential diagnostic value in distinguishing hypothalamic from pituitary causes of gonadotropin deficiency.
Copyright © 2010 American Society for Reproductive Medicine. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Gonadotropins.2018 Mar 26. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012–. 2018 Mar 26. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012–. PMID: 31644163 Free Books & Documents. Review.
-
Sex steroid control of gonadotropin secretion in the human male. I. Effects of testosterone administration in normal and gonadotropin-releasing hormone-deficient men.J Clin Endocrinol Metab. 1991 Sep;73(3):609-20. doi: 10.1210/jcem-73-3-609. J Clin Endocrinol Metab. 1991. PMID: 1908484 Clinical Trial.
-
Risk factors for a suboptimal response to gonadotropin-releasing hormone agonist trigger during in vitro fertilization cycles.Fertil Steril. 2015 Sep;104(3):637-42. doi: 10.1016/j.fertnstert.2015.06.011. Epub 2015 Jul 3. Fertil Steril. 2015. PMID: 26149355
-
Pulsatile gonadotropin secretion after discontinuation of long term gonadotropin-releasing hormone (GnRH) administration in a subset of GnRH-deficient men.J Clin Endocrinol Metab. 1989 Aug;69(2):377-85. doi: 10.1210/jcem-69-2-377. J Clin Endocrinol Metab. 1989. PMID: 2502554
-
Exaggerated free alpha-subunit levels during pulsatile gonadotropin-releasing hormone replacement in women with idiopathic hypogonadotropic hypogonadism.J Clin Endocrinol Metab. 1998 Jan;83(1):241-7. doi: 10.1210/jcem.83.1.4488. J Clin Endocrinol Metab. 1998. PMID: 9435449 Clinical Trial.
Cited by
-
The Pathogenesis of Polycystic Ovary Syndrome (PCOS): The Hypothesis of PCOS as Functional Ovarian Hyperandrogenism Revisited.Endocr Rev. 2016 Oct;37(5):467-520. doi: 10.1210/er.2015-1104. Epub 2016 Jul 26. Endocr Rev. 2016. PMID: 27459230 Free PMC article. Review.
-
Evidence that obesity and androgens have independent and opposing effects on gonadotropin production from puberty to maturity.Brain Res. 2010 Dec 10;1364:186-97. doi: 10.1016/j.brainres.2010.08.088. Epub 2010 Sep 25. Brain Res. 2010. PMID: 20816944 Free PMC article. Review.
-
Clinical review: Adolescent anovulation: maturational mechanisms and implications.J Clin Endocrinol Metab. 2013 Sep;98(9):3572-83. doi: 10.1210/jc.2013-1770. Epub 2013 Aug 2. J Clin Endocrinol Metab. 2013. PMID: 23913942 Free PMC article. Review.
-
The Effect of the Testis on the Ovary: Structure-Function Relationships in a Neonate with a Unilateral Ovotestis (Ovotesticular Disorder of Sex Development) .Horm Res Paediatr. 2017;87(3):205-212. doi: 10.1159/000455142. Epub 2017 Mar 2. Horm Res Paediatr. 2017. PMID: 28253506 Free PMC article.
-
Comparison of detection of normal puberty in boys by a hormonal sleep test and a gonadotropin-releasing hormone agonist test.J Clin Endocrinol Metab. 2012 Dec;97(12):4596-604. doi: 10.1210/jc.2012-2722. Epub 2012 Oct 5. J Clin Endocrinol Metab. 2012. PMID: 23043188 Free PMC article. Clinical Trial.
References
-
- Reitano JF, Caminos-Torres R, Snyder PJ. Serum LH and FSH responses to the repetitive administration of gonadotropin-releasing hormone in patients with idiopathic hypogonadotropic hypogonadism. J Clin Endocrinol Metab. 1975;41:1035–42. - PubMed
-
- Yoshimoto Y, Moridera K, Imura H. Restoration of normal pituitary gonadotropin reserve by administration of luteinizing-hormone-releasing hormone in patients with hypogonadotropic hypogonadism. N Engl J Med. 1975;292:242–5. - PubMed
-
- Ghai K, Cara JF, Rosenfield RL. Gonadotropin releasing hormone agonist (nafarelin) test to differentiate gonadotropin deficiency from constitutionally delayed puberty in teen-age boys--a clinical research center study. J Clin Endocrinol Metab. 1995;80:2980–6. - PubMed
-
- Ehrmann DA, Rosenfield RL, Cuttler L, Burstein S, Cara JF, Levitsky LL. A new test of combined pituitary-testicular function using the gonadotropin-releasing hormone agonist nafarelin in the differentiation of gonadotropin deficiency from delayed puberty: pilot studies. J Clin Endocrinol Metab. 1989;69:963–7. - PubMed
-
- Hoffman AR, Crowley WF., Jr Induction of puberty in men by long-term pulsatile administration of low-dose gonadotropin-releasing hormone. N Engl J Med. 1982;307:1237–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
