

Potential diagnostic utility of intermittent administration of short-acting gonadotropin-releasing hormone agonist in gonadotropin deficiency
- PMID: 20553679
- PMCID: PMC2944005
- DOI: 10.1016/j.fertnstert.2010.04.019
Potential diagnostic utility of intermittent administration of short-acting gonadotropin-releasing hormone agonist in gonadotropin deficiency
Abstract
Objective: To determine if intermittent, low-dose, short-acting gonadotropin-releasing hormone agonist (GnRH-agonist) administration sufficiently up-regulates pituitary-gonadal function in gonadotropin deficiency to be of diagnostic or therapeutic value.
Design: Case-control study.
Setting: General clinical research center.
Patient(s): Normal adult volunteers and gonadotropin-deficiency patients.
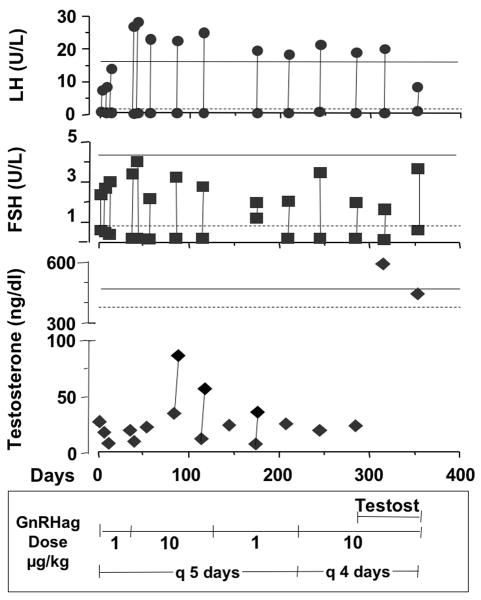
Intervention(s): Low-dose leuprolide acetate administered subcutaneously at 4- to 5-day intervals up to 1 year.
Main outcome measure(s): Levels of luteinizing hormone (LH), follicle-stimulating hormone (FSH), and sex steroid responses.
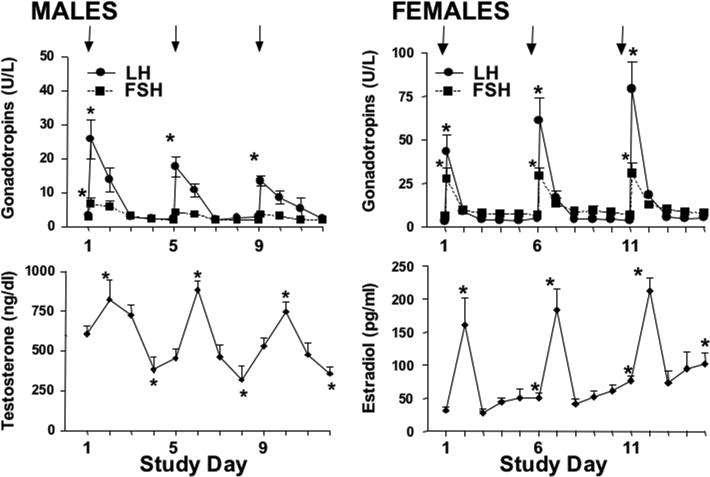
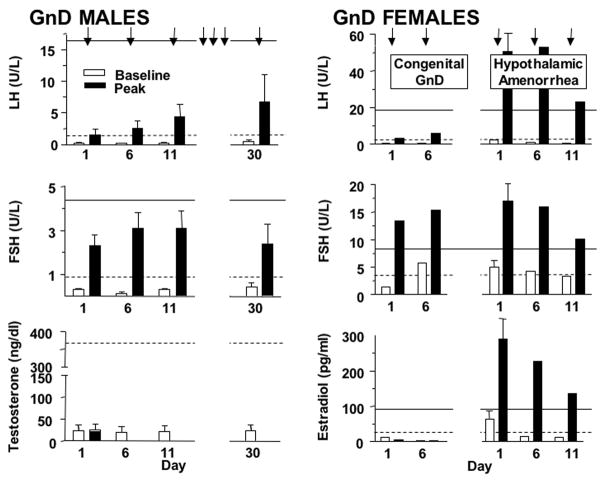
Result(s): In normal men and women, low-dose GnRH-agonist repetitively transiently stimulated gonadotropins in a gender-dimorphic manner. In congenitally gonadotropin-deficient men (n = 6) and women (n = 1), none of whom had a normal LH response to an initial GnRH-agonist test dose, this regimen consistently stimulated LH to the normal baseline range within 2 weeks. Long-term GnRH-agonist administration to a partially gonadotropin-deficient man did not alleviate hypogonadism, however. Women with hypothalamic amenorrhea (n = 2) responded normally to a single GnRH-agonist injection; however, repeated dosing did not seem to induce the normal priming effect.
Conclusion(s): The subnormal LH response to GnRH-agonist in patients with congenital gonadotropin deficiency normalized in response to repetitive intermittent GnRH-agonist administration but not sufficiently to improve hypogonadism. Hypothalamic amenorrhea patients lacked the priming response to repeated GnRH-agonist but otherwise had normal hormonal responses to GnRH-agonist. We conclude that intermittent administration of a short-acting GnRH-agonist is of potential diagnostic value in distinguishing hypothalamic from pituitary causes of gonadotropin deficiency.
Copyright © 2010 American Society for Reproductive Medicine. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Reitano JF, Caminos-Torres R, Snyder PJ. Serum LH and FSH responses to the repetitive administration of gonadotropin-releasing hormone in patients with idiopathic hypogonadotropic hypogonadism. J Clin Endocrinol Metab. 1975;41:1035–42. - PubMed
-
- Yoshimoto Y, Moridera K, Imura H. Restoration of normal pituitary gonadotropin reserve by administration of luteinizing-hormone-releasing hormone in patients with hypogonadotropic hypogonadism. N Engl J Med. 1975;292:242–5. - PubMed
-
- Ghai K, Cara JF, Rosenfield RL. Gonadotropin releasing hormone agonist (nafarelin) test to differentiate gonadotropin deficiency from constitutionally delayed puberty in teen-age boys--a clinical research center study. J Clin Endocrinol Metab. 1995;80:2980–6. - PubMed
-
- Ehrmann DA, Rosenfield RL, Cuttler L, Burstein S, Cara JF, Levitsky LL. A new test of combined pituitary-testicular function using the gonadotropin-releasing hormone agonist nafarelin in the differentiation of gonadotropin deficiency from delayed puberty: pilot studies. J Clin Endocrinol Metab. 1989;69:963–7. - PubMed
-
- Hoffman AR, Crowley WF., Jr Induction of puberty in men by long-term pulsatile administration of low-dose gonadotropin-releasing hormone. N Engl J Med. 1982;307:1237–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
