

Stress cardiac magnetic resonance imaging with observation unit care reduces cost for patients with emergent chest pain: a randomized trial
- PMID: 20554078
- PMCID: PMC3716462
- DOI: 10.1016/j.annemergmed.2010.04.009
Stress cardiac magnetic resonance imaging with observation unit care reduces cost for patients with emergent chest pain: a randomized trial
Abstract
Study objective: We determine whether imaging with cardiac magnetic resonance imaging (MRI) in an observation unit would reduce medical costs among patients with emergent non-low-risk chest pain who otherwise would be managed with an inpatient care strategy.
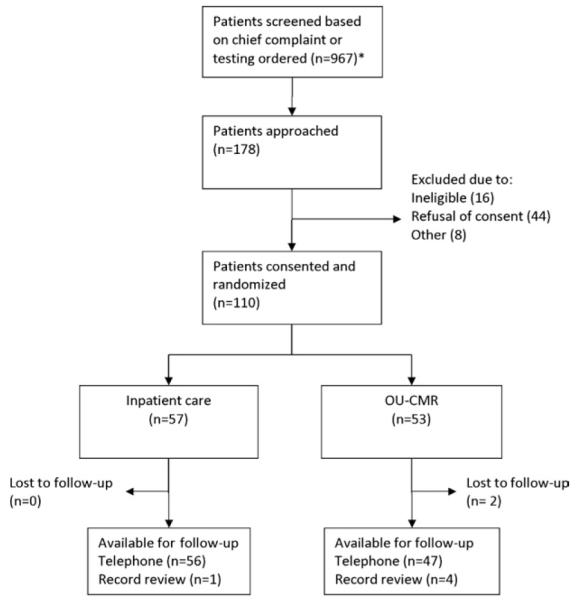
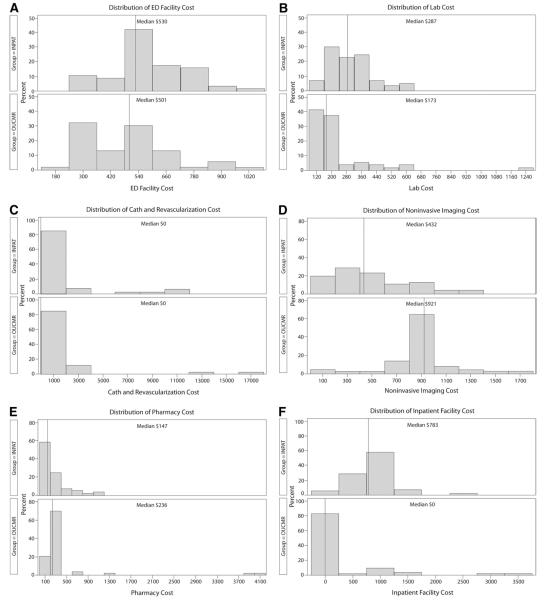
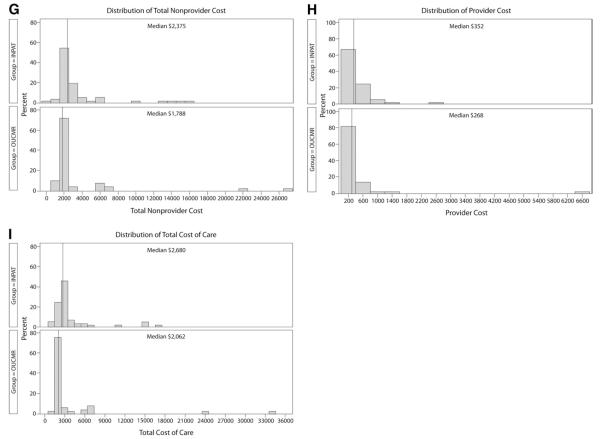
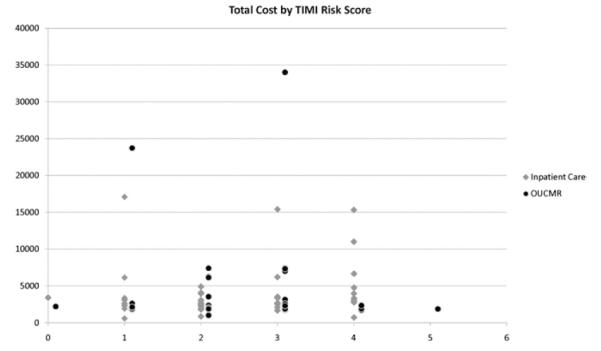
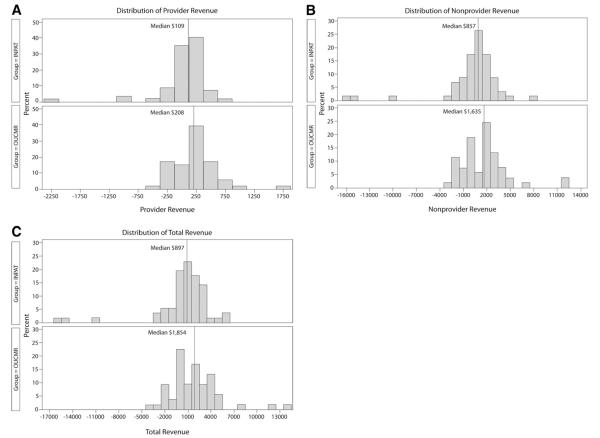
Methods: Emergency department patients (n=110) at intermediate or high probability for acute coronary syndrome without electrocardiographic or biomarker evidence of a myocardial infarction provided consent and were randomized to stress cardiac MRI in an observation unit versus standard inpatient care. The primary outcome was direct hospital cost calculated as the sum of hospital and provider costs. Estimated median cost differences (Hodges-Lehmann) and distribution-free 95% confidence intervals (Moses) were used to compare groups.
Results: There were 110 participants with 53 randomized to cardiac MRI and 57 to inpatient care; 8 of 110 (7%) experienced acute coronary syndrome. In the MRI pathway, 49 of 53 underwent stress cardiac MRI, 11 of 53 were admitted, 1 left against medical advice, 41 were discharged, and 2 had acute coronary syndrome. In the inpatient care pathway, 39 of 57 patients initially received stress testing, 54 of 57 were admitted, 3 left against medical advice, and 6 had acute coronary syndrome. At 30 days, no subjects in either group experienced acute coronary syndrome after discharge. The cardiac MRI group had a reduced median hospitalization cost (Hodges-Lehmann estimate $588; 95% confidence interval $336 to $811); 79% were managed without hospital admission.
Conclusion: Compared with inpatient care, an observation unit strategy involving stress cardiac MRI reduced incident cost without any cases of missed acute coronary syndrome in patients with emergent chest pain.
Copyright (c) 2010 American College of Emergency Physicians. Published by Mosby, Inc. All rights reserved.
Figures
Similar articles
-
Provider-directed imaging stress testing reduces health care expenditures in lower-risk chest pain patients presenting to the emergency department.Circ Cardiovasc Imaging. 2012 Jan;5(1):111-8. doi: 10.1161/CIRCIMAGING.111.965293. Epub 2011 Nov 29. Circ Cardiovasc Imaging. 2012. PMID: 22128195 Free PMC article. Clinical Trial.
-
Stress CMR imaging observation unit in the emergency department reduces 1-year medical care costs in patients with acute chest pain: a randomized study for comparison with inpatient care.JACC Cardiovasc Imaging. 2011 Aug;4(8):862-70. doi: 10.1016/j.jcmg.2011.04.016. JACC Cardiovasc Imaging. 2011. PMID: 21835378 Free PMC article. Clinical Trial.
-
Cost burden of non-specific chest pain admissions.Ir J Med Sci. 2013 Mar;182(1):57-61. doi: 10.1007/s11845-012-0826-5. Epub 2012 May 3. Ir J Med Sci. 2013. PMID: 22552895
-
Chest pain centers: diagnosis of acute coronary syndromes.Ann Emerg Med. 2000 May;35(5):449-61. Ann Emerg Med. 2000. PMID: 10783407 Review.
-
Evaluation of chest pain in the emergency department.Curr Probl Cardiol. 1997 Apr;22(4):149-236. doi: 10.1016/s0146-2806(97)80007-2. Curr Probl Cardiol. 1997. PMID: 9107535 Review.
Cited by
-
Rate and Causes of Discharge against Medical Advice in Iranian Hospitals: A Systematic Review and Meta-Analysis.Iran J Public Health. 2015 Jul;44(7):902-12. Iran J Public Health. 2015. PMID: 26576368 Free PMC article. Review.
-
Cost analysis of the History, ECG, Age, Risk factors, and initial Troponin (HEART) Pathway randomized control trial.Am J Emerg Med. 2017 Jan;35(1):77-81. doi: 10.1016/j.ajem.2016.10.005. Epub 2016 Oct 5. Am J Emerg Med. 2017. PMID: 27765481 Free PMC article.
-
Superior diagnostic performance of perfusion-cardiovascular magnetic resonance versus SPECT to detect coronary artery disease: The secondary endpoints of the multicenter multivendor MR-IMPACT II (Magnetic Resonance Imaging for Myocardial Perfusion Assessment in Coronary Artery Disease Trial).J Cardiovasc Magn Reson. 2012 Sep 2;14(1):61. doi: 10.1186/1532-429X-14-61. J Cardiovasc Magn Reson. 2012. PMID: 22938651 Free PMC article. Clinical Trial.
-
Provider-directed imaging stress testing reduces health care expenditures in lower-risk chest pain patients presenting to the emergency department.Circ Cardiovasc Imaging. 2012 Jan;5(1):111-8. doi: 10.1161/CIRCIMAGING.111.965293. Epub 2011 Nov 29. Circ Cardiovasc Imaging. 2012. PMID: 22128195 Free PMC article. Clinical Trial.
-
Role of cardiac magnetic resonance in the evaluation of dilated cardiomyopathy: diagnostic contribution and prognostic significance.ISRN Radiol. 2014 Feb 4;2014:365404. doi: 10.1155/2014/365404. eCollection 2014. ISRN Radiol. 2014. PMID: 24967294 Free PMC article. Review.
References
-
- Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol. 2007;50:e1–e157. - PubMed
-
- Gomberg-Maitland M, Murphy SA, Moliterno DJ, et al. Are we appropriately triaging patients with unstable angina? Am Heart J. 2005;149:613–618. - PubMed
-
- Tatum JL, Jesse RL, Kontos MC, et al. Comprehensive strategy for the evaluation and triage of the chest pain patient. Ann Emerg Med. 1997;29:116–125. - PubMed
-
- Stowers SA, Eisenstein EL, Wackers FJ, et al. An economic analysis of an aggressive diagnostic strategy with single photon emission computed tomography myocardial perfusion imaging and early exercise stress testing in emergency department patients who present with chest pain but nondiagnostic electrocardiograms: results from a randomized trial. Ann Emerg Med. 2000;35:17–25. - PubMed
-
- Nagel E, Lehmkuhl HB, Bocksch W, et al. Noninvasive diagnosis of ischemia-induced wall motion abnormalities with the use of high-dose dobutamine stress MRI: comparison with dobutamine stress echocardiography. Circulation. 1999;99:763–770. - PubMed
