

Asymptomatic embolisation for prediction of stroke in the Asymptomatic Carotid Emboli Study (ACES): a prospective observational study
- PMID: 20554250
- PMCID: PMC2890862
- DOI: 10.1016/S1474-4422(10)70120-4
Asymptomatic embolisation for prediction of stroke in the Asymptomatic Carotid Emboli Study (ACES): a prospective observational study
Abstract
Background: Whether surgery is beneficial for patients with asymptomatic carotid stenosis is controversial. Better methods of identifying patients who are likely to develop stroke would improve the risk-benefit ratio for carotid endarterectomy. We aimed to investigate whether detection of asymptomatic embolic signals by use of transcranial doppler (TCD) could predict stroke risk in patients with asymptomatic carotid stenosis.
Methods: The Asymptomatic Carotid Emboli Study (ACES) was a prospective observational study in patients with asymptomatic carotid stenosis of at least 70% from 26 centres worldwide. To detect the presence of embolic signals, patients had two 1 h TCD recordings from the ipsilateral middle cerebral artery at baseline and one 1 h recording at 6, 12, and 18 months. Patients were followed up for 2 years. The primary endpoint was ipsilateral stroke and transient ischaemic attack. All recordings were analysed centrally by investigators masked to patient identity.
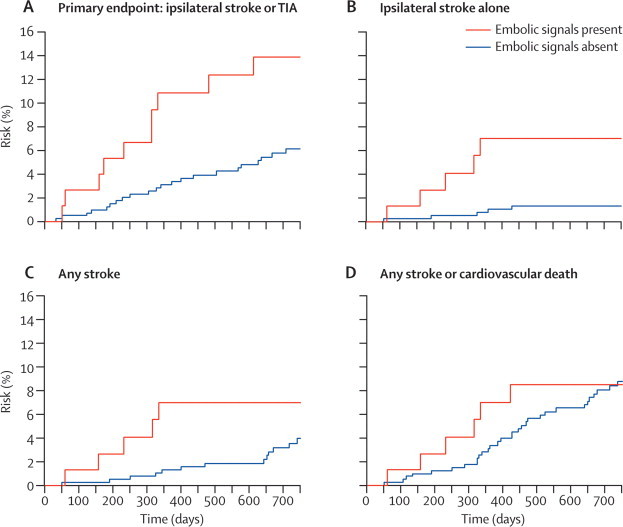
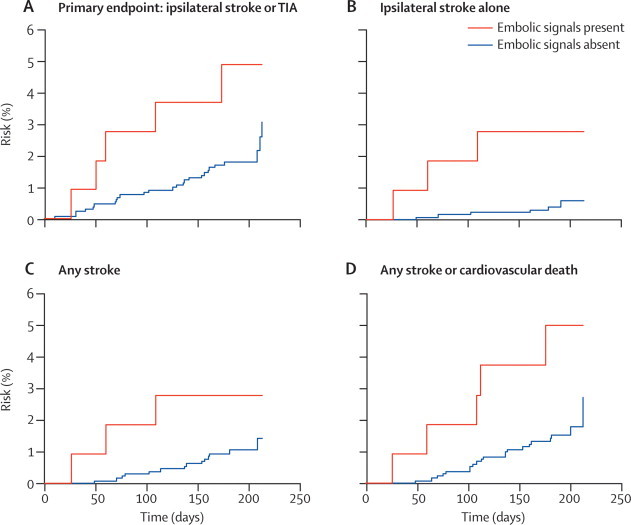
Findings: 482 patients were recruited, of whom 467 had evaluable recordings. Embolic signals were present in 77 of 467 patients at baseline. The hazard ratio for the risk of ipsilateral stroke and transient ischaemic attack from baseline to 2 years in patients with embolic signals compared with those without was 2.54 (95% CI 1.20-5.36; p=0.015). For ipsilateral stroke alone, the hazard ratio was 5.57 (1.61-19.32; p=0.007). The absolute annual risk of ipsilateral stroke or transient ischaemic attack between baseline and 2 years was 7.13% in patients with embolic signals and 3.04% in those without, and for ipsilateral stroke was 3.62% in patients with embolic signals and 0.70% in those without. The hazard ratio for the risk of ipsilateral stroke and transient ischaemic attack for patients who had embolic signals on the recording preceding the next 6-month follow-up compared with those who did not was 2.63 (95% CI 1.01-6.88; p=0.049), and for ipsilateral stroke alone the hazard ratio was 6.37 (1.59-25.57; p=0.009). Controlling for antiplatelet therapy, degree of stenosis, and other risk factors did not alter the results.
Interpretation: Detection of asymptomatic embolisation on TCD can be used to identify patients with asymptomatic carotid stenosis who are at a higher risk of stroke and transient ischaemic attack, and also those with a low absolute stroke risk. Assessment of the presence of embolic signals on TCD might be useful in the selection of patients with asymptomatic carotid stenosis who are likely to benefit from endarterectomy.
Funding: British Heart Foundation.
Copyright 2010 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Cerebral microemboli: smoking gun or innocent bystanders?Lancet Neurol. 2010 Jul;9(7):644-5. doi: 10.1016/S1474-4422(10)70138-1. Epub 2010 Jun 9. Lancet Neurol. 2010. PMID: 20542738 No abstract available.
-
Stroke: embolus detection could predict risk of stroke.Nat Rev Neurol. 2010 Aug;6(8):412. doi: 10.1038/nrneurol.2010.96. Nat Rev Neurol. 2010. PMID: 20718113 No abstract available.
-
Emboli detection in asymptomatic carotid stenosis.Lancet Neurol. 2010 Oct;9(10):948-9; author reply 949. doi: 10.1016/S1474-4422(10)70228-3. Lancet Neurol. 2010. PMID: 20864044 No abstract available.
-
Emboli detection in asymptomatic carotid stenosis.Lancet Neurol. 2010 Oct;9(10):948; author reply 949. doi: 10.1016/S1474-4422(10)70227-1. Lancet Neurol. 2010. PMID: 20864045 No abstract available.
References
-
- Rothwell PM, Eliasziw M, Gutnikov SA, Warlow CP, Barnett HJ, for the Carotid Endarterectomy Trialists Collaboration Endarterectomy for symptomatic carotid stenosis in relation to clinical subgroups and timing of surgery. Lancet. 2004;363:915–924. - PubMed
-
- Abbott AL, Bladin C, Levi C, Chambers B. What should we do about asymptomatic carotid stenosis? Int J Stroke. 2007;2:27–39. - PubMed
-
- Asymptomatic Carotid Atherosclerosis Study Group Carotid endarterectomy for patients with asymptomatic internal carotid artery stenosis. JAMA. 1995;273:1421–1428. - PubMed
-
- Halliday A, Mansfield A, Marro J, MRC Asymptomatic Carotid Surgery Trial (ACST) Collaborative Group Prevention of disabling and fatal strokes by successful carotid endarterectomy in patients without recent neurological symptoms: randomised controlled trial. Lancet. 2004;363:1491–1502. - PubMed
-
- Naylor AR, Gaines PA, Rothwell PM. Who benefits most from intervention for asymptomatic carotid stenosis: patients or professionals? Eur J Vasc Endovasc Surg. 2009;37:625–632. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
