

Effect of calcium supplementation in pregnancy on maternal bone outcomes in women with a low calcium intake
- PMID: 20554790
- PMCID: PMC3994635
- DOI: 10.3945/ajcn.2010.29217
Effect of calcium supplementation in pregnancy on maternal bone outcomes in women with a low calcium intake
Abstract
Background: Mobilization of maternal bone mineral partly supplies calcium for fetal and neonatal bone growth and development.
Objective: We investigated whether pregnant women with low calcium intakes may have a more extensive skeletal response postpartum that may compromise their short- or long-term bone health.
Design: In a subset of participants (n = 125) in a double-blind, randomized, placebo-controlled trial (International Trial Registry: ISRCTN96502494) in pregnant women in The Gambia, West Africa, with low calcium intakes (approximately 350 mg Ca/d), we measured bone mineral status of the whole body, lumbar spine, and hip by using dual-energy X-ray absorptiometry and measured bone mineral status of the forearm by using single-photon absorptiometry at 2, 13, and 52 wk lactation. We collected blood and urine from the subjects at 20 wk gestation and at 13 wk postpartum. Participants received calcium carbonate (1500 mg Ca/d) or a matching placebo from 20 wk gestation to parturition; participants did not consume supplements during lactation.
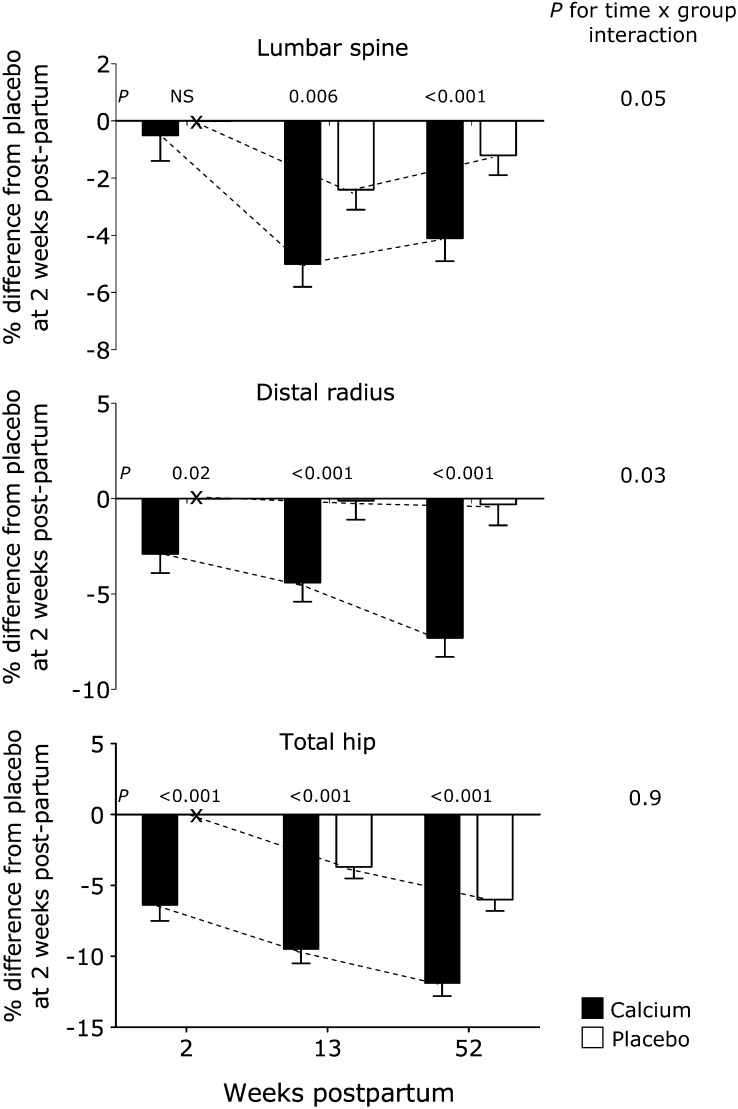
Results: Women who received the calcium supplement in pregnancy had significantly lower bone mineral content (BMC), bone area (BA), and bone mineral density (BMD) at the hip throughout 12 mo lactation (mean +/- SE difference: BMC = -10.7 +/- 3.7%, P = 0.005; BA = -3.8 +/- 1.9%, P = 0.05; BMD = -6.9 +/- 2.6%, P = 0.01). The women also experienced greater decreases in bone mineral during lactation at the lumbar spine and distal radius and had biochemical changes consistent with greater bone mineral mobilization.
Conclusions: Calcium supplementation in pregnant women with low calcium intakes may disrupt metabolic adaptation and may not benefit maternal bone health. Further study is required to determine if such effects persist long term or elicit compensatory changes in bone structure.
Figures
References
-
- Olausson H, Laskey MA, Goldberg GR, Prentice A. Changes in bone mineral status and bone size during pregnancy, and the influences of body weight and calcium intake. Am J Clin Nutr 2008;88:1032–9 - PubMed
-
- Prentice A. Micronutrients and the bone mineral content of the mother, fetus and newborn. J Nutr 2003;133:1693S–9S - PubMed
-
- Prentice A. Pregnancy and lactation. : Pettifor J, Juppner H, Glorieux F, Pediatric bone: biology and diseases. London, United Kingdom: Academic Press, 2003:249–69
-
- Laskey MA, Prentice A. Bone mineral changes during and after lactation. Obstet Gynecol 1999;94:608–15 - PubMed
-
- Laskey MA, Prentice A, Hanratty LA, et al. Bone changes after 3 mo of lactation: influence of calcium intake, breast-milk output, and vitamin D-receptor genotype. Am J Clin Nutr 1998;67:685–92 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
