

Antiretroviral regimens in pregnancy and breast-feeding in Botswana
- PMID: 20554983
- PMCID: PMC2999916
- DOI: 10.1056/NEJMoa0907736
Antiretroviral regimens in pregnancy and breast-feeding in Botswana
Abstract
Background: The most effective highly active antiretroviral therapy (HAART) to prevent mother-to-child transmission of human immunodeficiency virus type 1 (HIV-1) in pregnancy and its efficacy during breast-feeding are unknown.
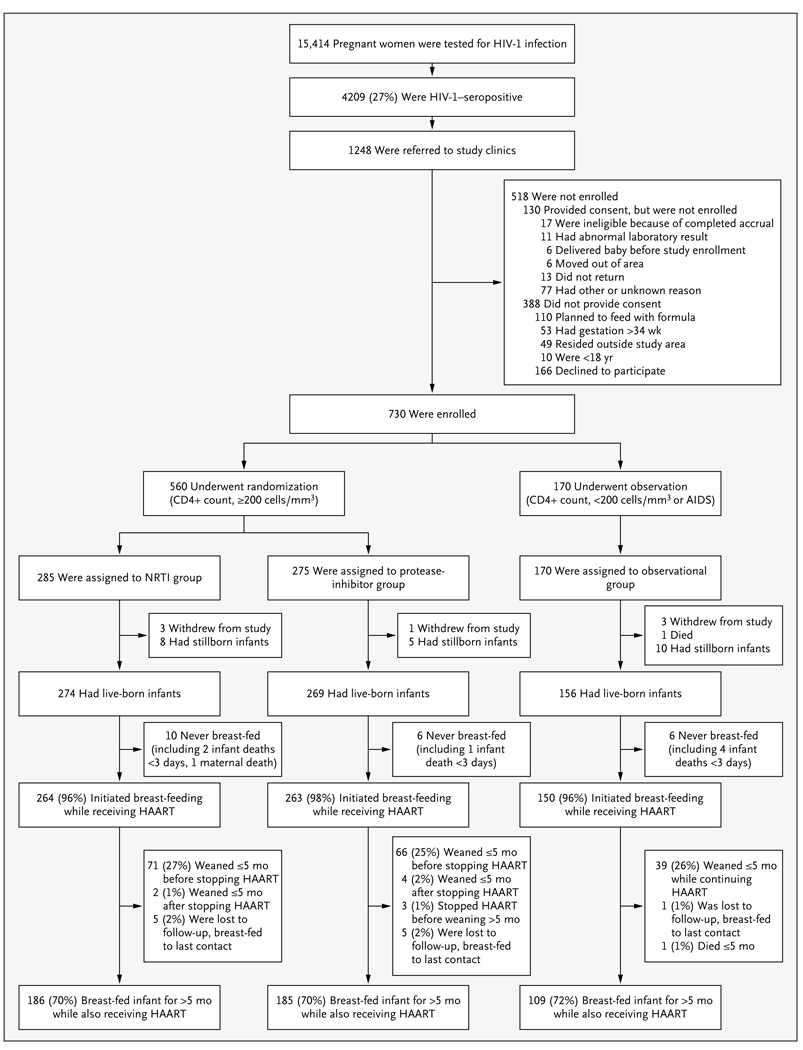
Methods: We randomly assigned 560 HIV-1-infected pregnant women (CD4+ count, > or = 200 cells per cubic millimeter) to receive coformulated abacavir, zidovudine, and lamivudine (the nucleoside reverse-transcriptase inhibitor [NRTI] group) or lopinavir-ritonavir plus zidovudine-lamivudine (the protease-inhibitor group) from 26 to 34 weeks' gestation through planned weaning by 6 months post partum. A total of 170 women with CD4+ counts of less than 200 cells per cubic millimeter received nevirapine plus zidovudine-lamivudine (the observational group). Infants received single-dose nevirapine and 4 weeks of zidovudine.
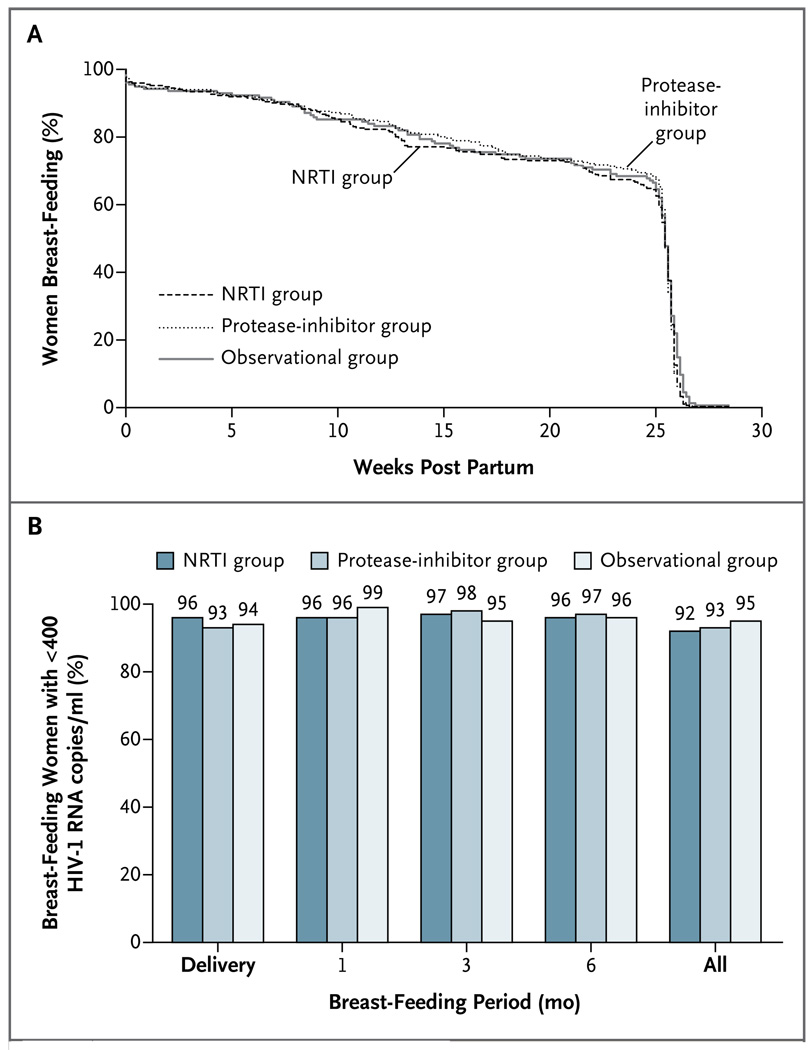
Results: The rate of virologic suppression to less than 400 copies per milliliter was high and did not differ significantly among the three groups at delivery (96% in the NRTI group, 93% in the protease-inhibitor group, and 94% in the observational group) or throughout the breast-feeding period (92% in the NRTI group, 93% in the protease-inhibitor group, and 95% in the observational group). By 6 months of age, 8 of 709 live-born infants (1.1%) were infected (95% confidence interval [CI], 0.5 to 2.2): 6 were infected in utero (4 in the NRTI group, 1 in the protease-inhibitor group, and 1 in the observational group), and 2 were infected during the breast-feeding period (in the NRTI group). Treatment-limiting adverse events occurred in 2% of women in the NRTI group, 2% of women in the protease-inhibitor group, and 11% of women in the observational group.
Conclusions: All regimens of HAART from pregnancy through 6 months post partum resulted in high rates of virologic suppression, with an overall rate of mother-to-child transmission of 1.1%. (ClinicalTrials.gov number, NCT00270296.)
2010 Massachusetts Medical Society
Figures
Comment in
-
Protecting the next generation--eliminating perinatal HIV-1 infection.N Engl J Med. 2010 Jun 17;362(24):2316-8. doi: 10.1056/NEJMe1004406. N Engl J Med. 2010. PMID: 20554987 No abstract available.
-
Maternal or infant antiretroviral drugs to reduce HIV-1 transmission.N Engl J Med. 2010 Nov 11;363(20):1969; author reply 1970. doi: 10.1056/NEJMc1009231. N Engl J Med. 2010. PMID: 21067395 No abstract available.
References
-
- Public Health Service Task Force. Recommendations for use of antiretroviral drugs in pregnant HIV-1 infected women for maternal health and interventions to reduce perinatal HIV transmission in the United States. [Accessed May 21, 2010]. (at http://aidsinfo.nih.gov/.) - PubMed
-
- Towards universal access: scaling up priority HIV/AIDS interventions in the health sector: progress report, April 2007. Geneva: World Health Organization; 2007.
-
- Antiretroviral drugs for treating pregnant women and preventing HIV infection in infants: towards universal access: recommendations for a public health approach — 2006 version. Geneva: World Health Organization; 2006. - PubMed
-
- Lockman S A5208/OCTANE Study Team. Lopinavir/ritonavir+tenofovir/emtricitabine is superior to nevirapine+tenofovir/emtricitabine for women with prior exposure to single-dose nevirapine: A5208 (OCTANE). Presented at the 16th Conference on Retroviruses and Opportunistic Infections; February 16–19, 2009; Montreal. abstract.
-
- DART Virology Group and Trial Team. Virological response to a triple nucleoside/nucleotide analogue regimen over 48 weeks in HIV-1-infected adults in Africa. AIDS. 2006;20:1391–1399. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials