

Normalization of urinary biomarkers to creatinine during changes in glomerular filtration rate
- PMID: 20555318
- PMCID: PMC3025699
- DOI: 10.1038/ki.2010.165
Normalization of urinary biomarkers to creatinine during changes in glomerular filtration rate
Abstract
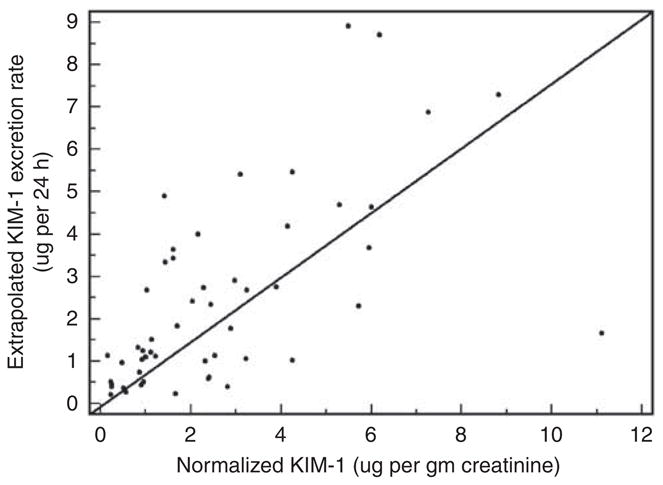
Urinary biomarkers, such as albumin and other markers of kidney injury, are frequently reported as a normalized ratio to urinary creatinine (UCr) concentration [UCr] to control for variations in urine flow rate. The implicit assumption is that UCr excretion is constant across and within individuals, such that changes in the ratio will reflect changes in biomarker excretion. Using computer simulations of creatinine kinetics, we found that normalized levels of a biomarker reflecting tubular injury can be influenced by dynamic changes in the UCr excretion rate when the glomerular filtration rate changes. Actual timed urine collections from hospitalized patients with changing glomerular filtration rates and/or critical illness exhibited variability in UCr excretion rates across and within individuals. Normalization by [UCr] may, therefore, result in an underestimation or overestimation of the biomarker excretion rate depending on the clinical context. Lower creatinine excretion in the setting of acute kidney injury or poor renal allograft function may amplify a tubular injury biomarker signal, thereby increasing its clinical utility. The variability of creatinine excretion, however, will complicate the determination of a threshold value for normalized biomarkers of acute or chronic kidney disease, including albumin. Thus, we suggest that the most accurate method to quantify biomarkers requires the collection of timed urine specimens to estimate the actual excretion rate, provided that the biomarker is stable over the period of collection. This ideal must be balanced, however, against practical considerations.
Figures




Comment in
-
Urinary kidney injury biomarkers and urine creatinine normalization: a false premise or not?Kidney Int. 2010 Sep;78(5):433-5. doi: 10.1038/ki.2010.200. Kidney Int. 2010. PMID: 20706215
References
-
- Han WK, Bailly V, Abichandani R, et al. Kidney injury molecule-1 (KIM-1): a novel biomarker for human renal proximal tubule injury. Kidney Int. 2002;62 :237–244. - PubMed
-
- Mishra J, Dent C, Tarabishi R, et al. Neutrophil gelatinase-associated lipocalin (NGAL) as a biomarker for acute renal injury after cardiac surgery. Lancet. 2005;365:1231–1238. - PubMed
-
- Parikh CR, Jani A, Melnikov VY, et al. Urinary interleukin-18 is a marker of human acute tubular necrosis. Am J Kidney Dis. 2004;43:405–414. - PubMed
-
- Liangos O, Perianayagam MC, Vaidya VS, et al. Urinary N-acetyl-beta-(D)-glucosaminidase activity and kidney injury molecule-1 level are associated with adverse outcomes in acute renal failure. J Am Soc Nephrol. 2007;18:904–912. - PubMed
-
- Washburn KK, Zappitelli M, Arikan AA, et al. Urinary interleukin-18 is an acute kidney injury biomarker in critically ill children. Nephrol Dial Transplant. 2008;23:566–572. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
