Radiographic and histologic response to neoadjuvant radiotherapy in patients with soft tissue sarcoma
- PMID: 20556523
- PMCID: PMC2941714
- DOI: 10.1245/s10434-010-1156-3
Radiographic and histologic response to neoadjuvant radiotherapy in patients with soft tissue sarcoma
Abstract
Background: Limited data exist regarding the radiographic and histologic response of soft tissue sarcoma (STS) to neoadjuvant radiotherapy (RT).
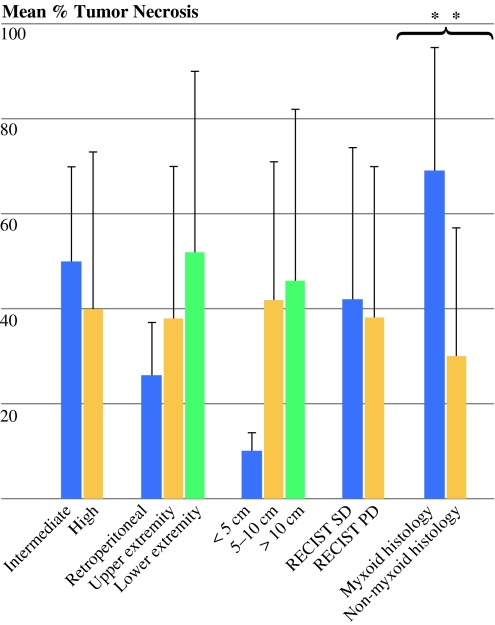
Methods: Between February 2000 and January 2009, a total of 25 patients aged >16 years with intermediate- or high-grade primary STS of all sites were treated with neoadjuvant RT followed by definitive resection. Patients receiving chemoradiotherapy were excluded. Cross-sectional images obtained before and after RT as well as pathologic specimens were reviewed for maximal change in tumor diameter and percentage tumor necrosis, respectively. Clinicopathologic variables were analyzed for their association with pathologic and radiographic response.
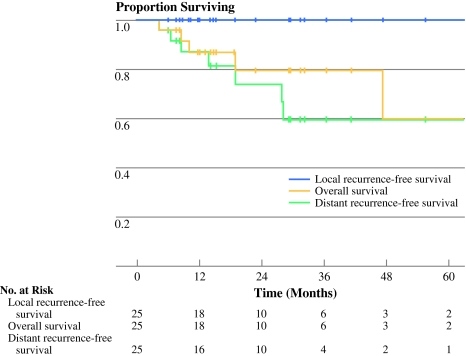
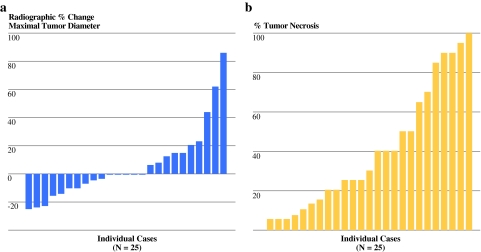
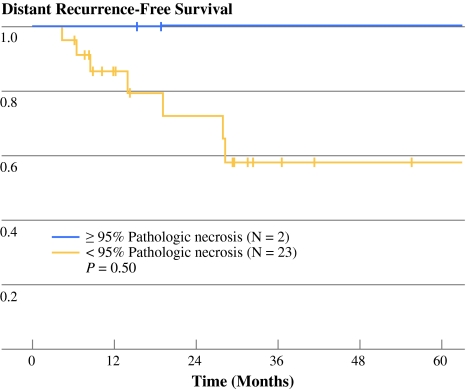
Results: There were 18 extremity (72%) and 7 retroperitoneal (28%) tumors. Median maximal tumor size was 9 cm (range, 3.3-35 cm), and 88% were of high grade. There were 21 R0 resections (84%) and 4 R1 resections (16%). Radiographically, the median percentage change in tumor diameter was 0% (range, -25 to +86%). By Response Evaluation Criteria in Solid Tumors (RECIST), 5 patients demonstrated progressive disease, 20 demonstrated stable disease, and 0 demonstrated partial/complete response. The median pathologic percentage tumor necrosis was 30% (range, 5-100%). Two tumors (8%) demonstrated near-complete pathologic response (≥95% necrosis). Near-complete pathologic response was associated with favorable oncologic outcomes, although these associations were not statistically significant.
Conclusions: Radiologic and near-complete pathologic responses are rare events after preoperative RT for STS. Near-complete pathologic response may be a potentially meaningful surrogate marker for disease outcome and is not predicted by RECIST response. Knowledge of these historical response rates is important for the evaluation of novel neoadjuvant therapies for patients with STS.
Figures