

Interventions for preventing blood loss during the treatment of cervical intraepithelial neoplasia
- PMID: 20556752
- PMCID: PMC4161495
- DOI: 10.1002/14651858.CD001421.pub2
Interventions for preventing blood loss during the treatment of cervical intraepithelial neoplasia
Update in
-
Interventions for preventing blood loss during the treatment of cervical intraepithelial neoplasia.Cochrane Database Syst Rev. 2013 Dec 4;2013(12):CD001421. doi: 10.1002/14651858.CD001421.pub3. Cochrane Database Syst Rev. 2013. PMID: 24302533 Free PMC article.
Abstract
Background: Cervical intraepithelial neoplasia (CIN) is the most common pre-malignant lesion. Surgical treatments for CIN are commonly associated with blood loss.
Objectives: To assess the effectiveness and safety of interventions for preventing blood loss during the treatment of CIN.
Search strategy: We searched the Cochrane Gynaecological Cancer Group Trials Register, MEDLINE, EMBASE and CENTRAL up to April 2009. We also searched registers of clinical trials, abstracts of scientific meetings and reference lists of included studies.
Selection criteria: Randomised controlled trials (RCTs) of vasopressin, tranexamic acid, haemostatic sutures, Amino-Cerv or Monsel's solution in women undergoing surgery for CIN.
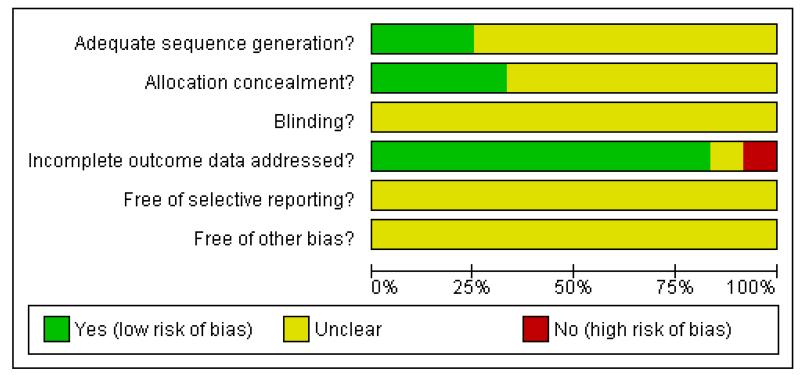
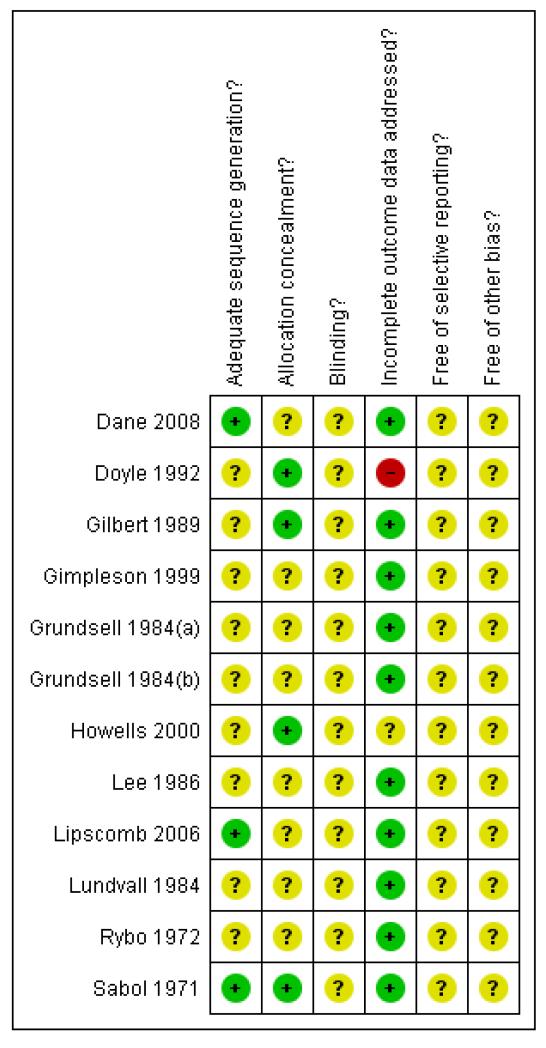
Data collection and analysis: Two reviewers independently abstracted data and assessed risk of bias. Risk ratios comparing adverse events in women who received one of the interventions were pooled in a random-effects meta-analyses or included in single trial analyses.
Main results: Twelve RCTs (N = 1602, of whom 1512 were assessed) were included.Vasopressin significantly reduced perioperative bleeding (mean difference (MD) = -100.80, 95% confidence interval (CI) -129.48 to -72.12) and was associated with a decreased risk of bleeding that required haemostatic sutures or further vasopressin, compared to placebo (risk ratio (RR) = 0.39, 95% CI 0.27 to 0.56).Tranexamic acid significantly reduced risk of secondary haemorrhage (RR = 0.23, 95% CI 0.11 to 0.50), but not primary haemorrhage (RR = 1.24, 95% CI 0.04 to 38.23) after knife and laser cone biopsy, compared with placebo. There was also a statistically significant reduction in postoperative blood loss compared with placebo (MD = -55.60, 95% CI -94.91 to -16.29).Packing with Monsel's solution resulted in less perioperative blood loss (MD = -22.00, 95% CI -23.09 to -20.91) and decreased the risk of dysmenorrhoea (RR = 0.37, 95% CI 0.16 to 0.84), unsatisfactory colposcopy (RR = 0.43, 95% CI 0.30 to 0.63) and cervical stenosis (RR = 0.35, 95% CI 0.25 to 0.49) compared to routine suturing, but was not statistically different to sutures for risk of primary and secondary haemorrhages.Amino-Cerv antibiotic gel failed to make a difference on secondary haemorrhage but was associated with significantly less vaginal discharge at 2 weeks compared with routine care (RR = 0.27, 95% CI 0.09 to 0.86).There was no significant difference in blood loss between women who received ball electrode diathermy and those who received Monsel's paste (MD = 4.82, 95% CI -3.45 to 13.09).
Authors' conclusions: Bleeding associated with surgery of the cervix appears to be reduced by vasopressin, used in combination with local anaesthetic. Tranexamic acid appears to be beneficial after knife and laser cone biopsy. There are insufficient data to assess the effects on primary haemorrhage. There is some evidence that haemostatic suturing has an adverse effect on blood loss, cervical stenosis and satisfactory colposcopy.
Figures
Update of
-
Interventions for preventing blood loss during the treatment of cervical intraepithelial neoplasia.Cochrane Database Syst Rev. 2000;(2):CD001421. doi: 10.1002/14651858.CD001421. Cochrane Database Syst Rev. 2000. Update in: Cochrane Database Syst Rev. 2010 Jun 16;(6):CD001421. doi: 10.1002/14651858.CD001421.pub2. PMID: 10796789 Updated.
References
References to studies included in this review
-
- Dane C, Dane B, Cetin A, Erginbas M. Haemostasis after cold-knife conisation: a randomised prospective trial comparing cerclage suture versus electro-cauterization. Australian and New Zealand Journal of Obstetrics and Gynaecology. 2008;48(3):343–7. - PubMed
-
- Doyle M, Warwick A, Redman C, Hillier C, Chenoy R, O’Brien S. Does application of Monsel’s solution after loop diathermy excision of the transformation zone reduce postoperative discharge? Results of a prospective randomised controlled trial. British Journal of Obstetrics and Gynaecology. 1992;99:1023–4. - PubMed
-
- Gilbert L, Saunders N, Stringer R, Sharp F. Hemostasis and cold knife cone biopsy: A prospective randomised trial comparing a suture versus non-suture technique. Obstetrics and Gynecology. 1989;74:640–3. - PubMed
-
- Gimpelson RJ, Graham B. Using Amino-Cerv after cervical LEEP. Journal of Reproductive Medicine. 1999;44(3):275–8. - PubMed
-
- Grundsell H, Larsson G, Bekassy Z. Use of an antifibrinolytic agent (tranexamic acid) and lateral sutures with laser conization of the cervix. Obstetrics and Gynecology. 1984;64:573–6. - PubMed
References to studies excluded from this review
-
- Chan KK, Tam KF, Tse KY, Ngan HY. The use of vaginal antimicrobial after large loop excision of transformation zone: a prospective randomised trial. BJOG. 2007;114(8):970–6. - PubMed
-
- Cruickshank ME, Anthony GB, Fitzmaurice A, McConnell D, Graham W, Alexander DA, et al. A randomised controlled trial to evaluate the effect of self-administered analgesia on women’s experience of outpatient treatment at colposcopy. BJOG. 2005;112(12):1652–8. - PubMed
-
- Foden-Shroff J, Redman CW, Tucker H, Millinship J, Thomas E, Warwick A, et al. Do routine antibiotics after loop diathermy excision reduce morbidity? BJOG. 1998;105(9):1022–5. - PubMed
-
- Harper DM. Paracervical block diminishes cramping associated with cryosurgery. Journal of Family Practice. 1997;44(1):71–5. - PubMed
-
- Paraskevaidis E, Koliopoulos G, Paschopoulos M, Stefanidis K, Navrozoglou I, Lolis D. Effects of ball cauterization following loop excision and follow-up colposcopy. Obstetrics and Gynaecology. 2001;97(4):617–20. - PubMed
Additional references
-
- Cirisano FD. Management of pre-invasive disease of the cervix. Seminars in Surgical Oncology. 1999;16(3):222–7. - PubMed
-
- Deeks JJ, Altman DG, Bradburn MJ. Statistical methods for examining heterogeneity and combining results from several studies in meta-analysis. In: Egger M, Davey Smith G, Altman DG, editors. Systematic Reviews in Health Care: Meta-Analysis in Context. 2nd Edition BMJ Publication Group; London: 2001.
-
- DerSimonian R, Laird N. Meta-analysis in clinical trials. Controlled Clinical Trials. 1986;7:177–88. - PubMed
-
- Sant M, Aareleid T, Berrino F, Bielska Lasota M, Carli PM, Faivre J, et al. EUROCARE-3: survival of cancer patients diagnosed 1990-94 - results and commentary. Annals of Oncology. 2003;14(Supplement 5):v61–v118. - PubMed
-
- Ferlay J, Bray F, Pisani P, Parkin DM, GLOBOCAN 2002 . IARC CancerBase No. 5. version 2.0 IARCPress; Lyon: 2004. Cancer incidence, mortality and prevalence worldwide.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous