

Interventions for sensory impairment in the upper limb after stroke
- PMID: 20556766
- PMCID: PMC6464855
- DOI: 10.1002/14651858.CD006331.pub2
Interventions for sensory impairment in the upper limb after stroke
Abstract
Background: Sensory impairments significantly limit the ability to use the upper limb after stroke. However, little is known about the effects of interventions used to address such impairments.
Objectives: To determine the effects of interventions that target upper limb sensory impairment after stroke.
Search strategy: We searched the Cochrane Stroke Group Trials Register (last searched 8 October 2009), the Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 2009, Issue 1), MEDLINE (1966 to January 2009), EMBASE (1980 to January 2009), and six further electronic databases to January 2009. We also handsearched relevant journals, contacted authors in the field, searched doctoral dissertation databases, checked reference lists, and completed citation tracking.
Selection criteria: Randomized controlled trials and controlled trials comparing interventions for sensory impairment after stroke with no treatment, conventional treatment, attention placebo or with other interventions for sensory impairment.
Data collection and analysis: Two review authors selected studies, assessed quality and extracted data. We analyzed study data using mean differences and odds ratios as appropriate. The primary outcome we considered was sensory function and secondary outcomes examined included upper limb function, activities of daily living, impact of stroke and quality of life as well as adverse events.
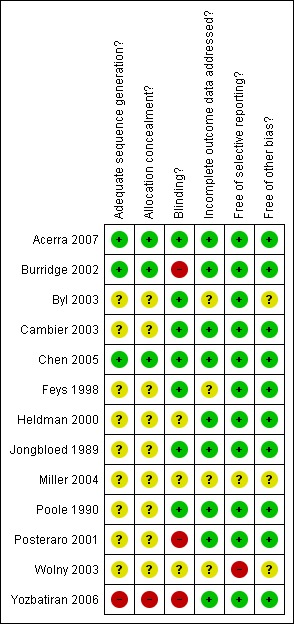
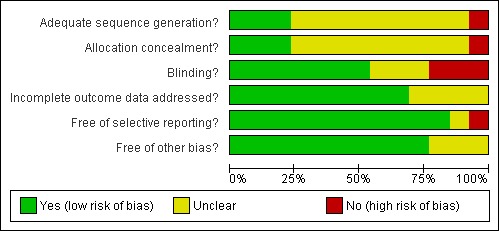
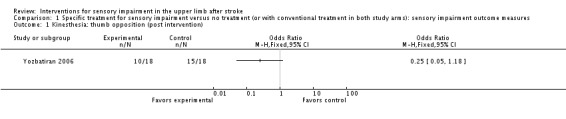
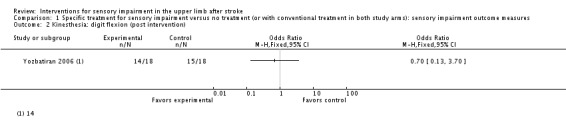
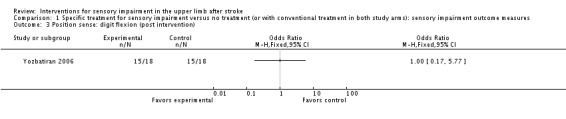
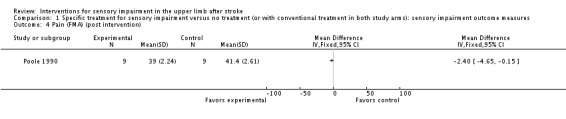
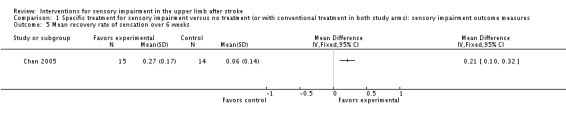
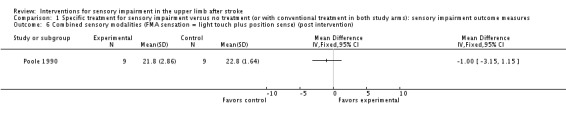
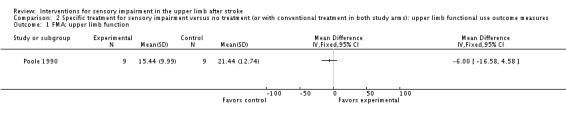
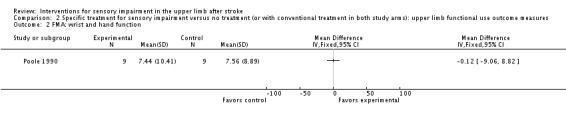
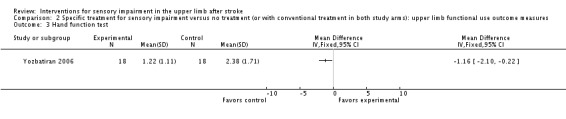
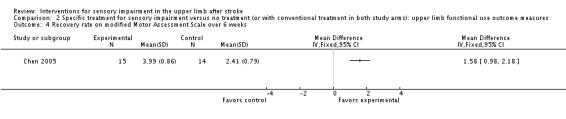
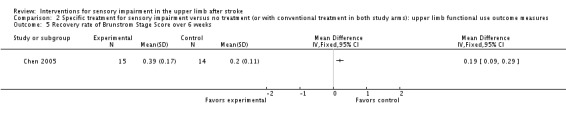
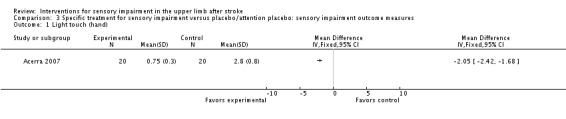
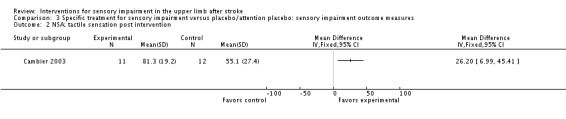
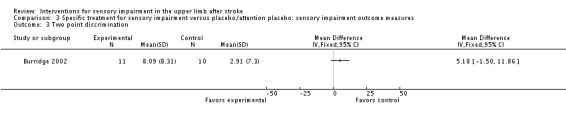
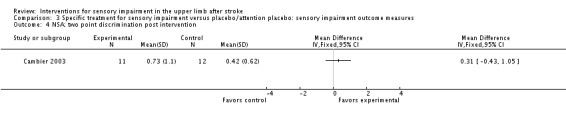
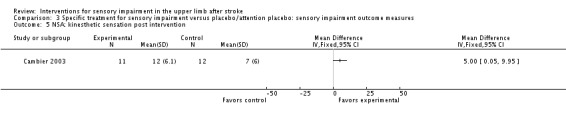
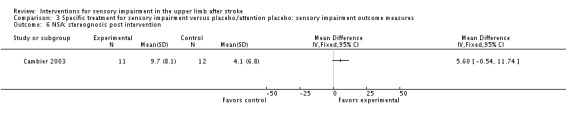
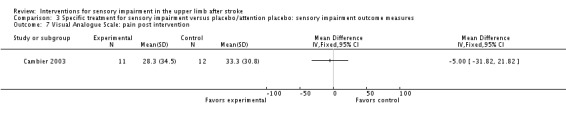
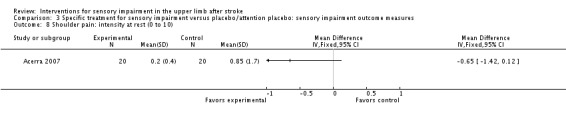
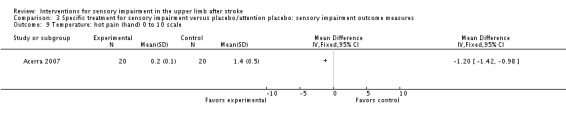
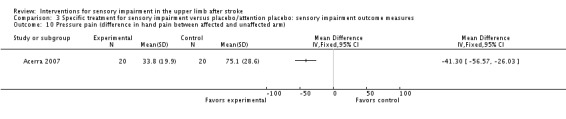
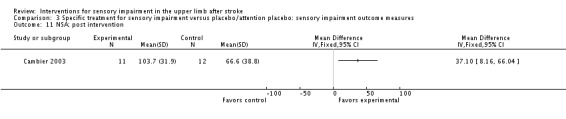
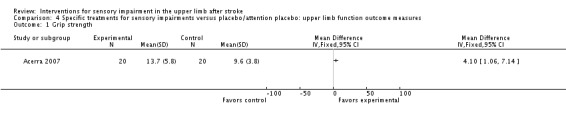
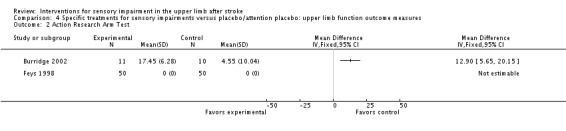
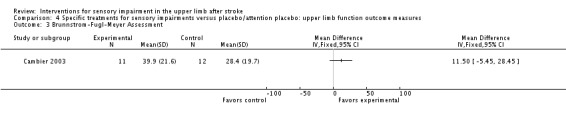
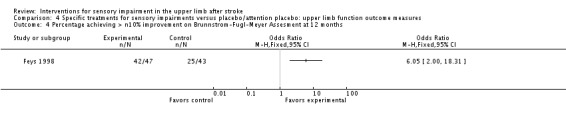
Main results: We included 13 studies, with a total 467 participants, testing a range of different interventions. Outcome measures included 36 measures of sensory impairment and 13 measures of upper limb function. All but two studies had unclear or high risk of bias. While there is insufficient evidence to reach conclusions about the effects of interventions included in this review, three studies provided preliminary evidence for the effects of some specific interventions, including mirror therapy for improving detection of light touch, pressure and temperature pain; a thermal stimulation intervention for improving rate of recovery of sensation; and intermittent pneumatic compression intervention for improving tactile and kinesthetic sensation. We could not perform meta-analysis due to a high degree of clinical heterogeneity in both interventions and outcomes.
Authors' conclusions: Multiple interventions for upper limb sensory impairment after stroke are described but there is insufficient evidence to support or refute their effectiveness in improving sensory impairment, upper limb function, or participants' functional status and participation. There is a need for more well-designed, better reported studies of sensory rehabilitation.
Conflict of interest statement
None known. Dr Kryss McKenna (deceased April 2009) had no known declarations of interest listed in the previously published protocol.
Figures
Update of
References
References to studies included in this review
-
- Acerra NE. Sensorimotor Dysfunction in CRPS1 and Stroke: Characterisation, Prediction and Intervention. Doctor of Philosophy Degree Thesis. University of Queensland, 2007.
- Acerra NE, Souvlis T, Moseley G. Does mirror‐box therapy improve sensory and motor changes in the early post‐stroke population? A randomised controlled trial. Australian Journal of Physiotherapy 2005;51(4‐e Suppl):S7.
-
- Burridge JH, Mann GE, Malone L, Taylor PN. A randomised controlled pilot study to investigate the effect of neuromuscular electrical stimulation on upper limb function following stroke. Proceedings of the 3rd World Congress in Neurological Rehabilitation April 2‐ 6. 2002.
- Burridge JH, Mann GE, Malone L, Taylor PN. A randomized controlled pilot study to investigate the effects of neuromuscular electrical stimulation on upper limb function following stroke. Neurorehabiliation and Neural Repair 2002;16(1):11.
- Mann G, Burridge JH, Malone LJ, Strike P. A pilot study to investigate the effects of electrical stimulation on recovery of hand function and sensation in subacute stroke patients. Neuromodulation 2005;3:193‐202. - PubMed
- Mann GE, Malone LJ, Taylor PN, Burridge JH. A randomised controlled pilot study to investigate the effect of neuromuscular electrical stimulation on upper limb function and hand sensation following stroke. 1st Annual Conference of FESnet September 2‐3. 2002.
-
- Byl N, Roderick J, Mohamed O, Hanny M, Kotler J, Smith A, et al. Effectiveness of sensory motor rehabilitation of the upper limb following the principles of neuroplasticity: patients stable poststroke. Neurorehabilitation and Neural Repair 2003;17(3):176‐91. - PubMed
-
- Cambier DC, Corte E, Danneels LA, Witvrouw EE. Treating sensory impairments in the post‐stroke upper limb with intermittent pneumatic compression. Results of a preliminary trial. Clinical Rehabilitation 2003;17:14‐20. - PubMed
-
- Chen JC, Liang CC, Shaw FZ. Facilitation of sensory and motor recovery by thermal intervention for the hemiplegic upper limb in acute stroke patients. Stroke 2005;36(12):2665‐9. - PubMed
References to studies excluded from this review
-
- Brogardh C, Sjolund B. Constraint induced movement therapy in patients with stroke: a pilot study on effects of small group training and of extended mitt use. Clinical Rehabilitation 2006;20:218‐27. - PubMed
-
- Carey L, Matyas T, Oke L. Sensory loss in stroke patients: effective training of tacticle and proprioceptive discrimination. Archives of Physical Medicine and Rehabilitation 1993;74(6):602‐11. - PubMed
-
- Liu W, Lipsitz LA, Montero‐Odasso M, Bean J, Kerrigan DC, Collins JJ. Noise‐enhanced vibrotactile sensitivity in older adults, patients with stroke, and patients with diabetic neuropathy. Archives of Physical Medicine and Rehabilitation 2002;83:171‐6. - PubMed
References to ongoing studies
-
- Ben‐Shabat E, Carey L, Brotchie PR. A brain activation study of limb position sense in stroke affected individuals with and without sensory training and in healthy aged. Royal Australian College of Physicians2006.
- Ben‐Shabat E, Carey LM, Matyas TA, Brotchie PR. A brain activation study of limb position sense in stroke affected individuals, with and without sensory training, and in healthy aged. Internal Medicine Journal 2006;36:A14.
-
- Carey L. Brain adaptation associated with spontaneous and training‐induced recovery of touch sensation post‐stroke. Australian New Zealand Clinical Trials Registry2004.
-
- Carey L. Effectiveness of training somatosensation in the hand after stroke: a randomized controlled trial. Australian New Zealand Clinical Trials Registry2002.
- Carey L. SENSE (Study of effectiveness of Neurorehabilitation on Sensation after Stroke): a randomized controlled trial. Internal Medicine Journal 2007;37 Suppl 1:A12.
Additional references
-
- Aruin AS. Support‐specific modulation of grip force in individuals with hemiparesis. Archives of Physical Medicine and Rehabilitation 2005;86(4):768‐75. - PubMed
-
- American Stroke Association. Impact of stroke. http://www.strokeassociation.org/presenter.jhtml?identifier=10332006.
-
- Aboriginal Stroke Project Steering Committee. National stroke unit program: Aboriginal stroke project. National Stroke Foundation of Australia, 2004.
-
- Blennerhassett JM, Matyas TA, Carey LM. Impaired discrimination of surface friction contributes to pinch grip deficit after stroke. Neurorehabilitation and Neural Repair 2007;21:263‐72. - PubMed
-
- Blumenfeld H. Neuroanatomy Through Clinical Cases. Sunderland, MA: Sinauer Associates, 2002.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical