

. 2008 Sep 1;14 Suppl 1(Suppl 1):63-74.
doi: 10.1177/15910199080140S112.
Epub 2008 Oct 9.
Complications of interventional treatment of cerebral aneurysms
Affiliations
- PMID: 20557777
- PMCID: PMC3328051
- DOI: 10.1177/15910199080140S112
Item in Clipboard
Complications of interventional treatment of cerebral aneurysms
Interv Neuroradiol.
.
No abstract available
Figures

A schematic outline of the clotting pathway and its interaction with platelets.. The site of action of the main antiplatelet and thrombolytic agents (adapted from R Laitt).

Clot forming on the coil ball (arrowhead).
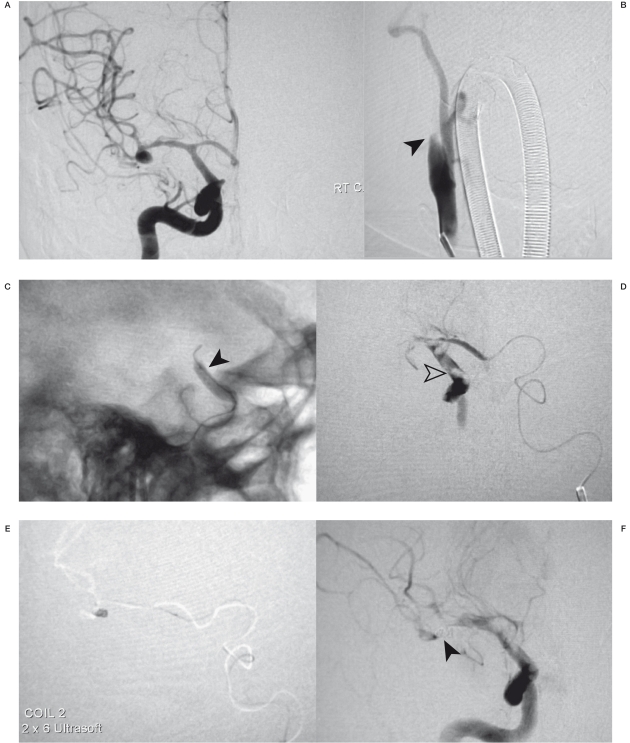
A) shows an MCA aneurysm with vasospam of MI. B) shows complete occlusion of the internal carotid (arrow); no evidence of dissection seen. C) balloon angioplasty arrow and clot retrieval failed in this case. D) catheterisation via the left carotid was performed and shows multiple thrombi (arrowhead) in the distal ICA and occlusion of the MCA. E) The aneurysm is being rapidly coiled from the left carotid approach. F) Reopro was then given with rapid recannalisation, note the residual spasm in the M1 (arrow) and clot in the distal ICA. Nimopodine 1 mg was given IA and good perfusion of the MCA was achieved. The patient had no clinical deficit after the procedure.

Proximal vertebral occlusion (A) secondary to dissection (arrow) (B) following thrombolysis this reoccluded and required stenting (C) distal embolus (arrow) in an MCA branch, see delayed collateral flow in the image below.

Distal embolus (arrow) in an MCA branch, good collateral flow to the affected region. This was managed with fluids and hypertension with no resultantclinical deficit.

Loss of the right posterior cerebral artery (A), salvage angioplasty (B) coil ball remodelled (C) with artery reopened.

Distal coil embolisation (arrow). Distal coil embolisation; the coil is acting like a stent and not obstructing flow.

Coil migration (A) the long tail of coil can be stented to the artery wall or retrieved in this case by a goose necked snare (B),

A small helical coil arrowhead (A) being retrieved by a Merci device (B).

A small narrow necked aneurysm (A) in combination with the very tortuous proximal cerebral vessels (B) this is a high risk of rupture situation. The catheter tip is placed too close to the wall of the dome of the aneurysm. The coil and catheter in this situation often have stored energy (C) which over time releases into the aneurysm causing rupture (D)

There is a dissected right vertebral artery with two distict aneurysms (arrows) (A). Stenting followed by coiling the aneurysm has resulted in rupture (arrow) (B) Normally this would have been treated by parent vessel occlusion but the left subclavian was completely occluded.

Patient with a right cavernous carotid aneurysm with severe peri-orbital pain (A). The contra-lateral carotid angiogram performed whilst left carotid balloon inflated; no cross-flow across the anterior communicating artery noted. (B) Patient "passed" balloon occlusion test clinically but the small posterior communicating artery < 1.5 mm is worrying and a hypotensive challenge would have been useful. Patient had a stroke 12 hrs post occlusion. (c) A left vertebral injection shows filling of the right hemisphere arteries with no significant arterial or venous delay. Note that the posterior communicating artery is less that 1.5 mm in diameter.
Similar articles
-
Reporting standards for endovascular repair of saccular intracranial cerebral aneurysms.J Neurointerv Surg. 2010 Dec;2(4):312-23. doi: 10.1136/jnis.2010.002337. Epub 2010 Sep 21. J Neurointerv Surg. 2010. PMID: 21990640
-
Reporting standards for endovascular repair of saccular intracranial cerebral aneurysms.J Vasc Interv Radiol. 2009 Jul;20(7 Suppl):S435-50. doi: 10.1016/j.jvir.2009.03.004. J Vasc Interv Radiol. 2009. PMID: 19560031
-
Three-year experience with interventional neuroradiology for management of cerebral aneurysms at a single Australian centre.J Med Imaging Radiat Oncol. 2018 Feb;62(1):51-56. doi: 10.1111/1754-9485.12634. Epub 2017 Jul 20. J Med Imaging Radiat Oncol. 2018. PMID: 28726260
-
Reporting standards for endovascular repair of saccular intracranial cerebral aneurysms.Stroke. 2009 May;40(5):e366-79. doi: 10.1161/STROKEAHA.108.527572. Epub 2009 Feb 26. Stroke. 2009. PMID: 19246711 Review.
-
Intracranial aneurysms in sickle cell disease: Aneurysms characteristics and modalities of endovascular approach to treat these patients.J Neuroradiol. 2020 May;47(3):221-226. doi: 10.1016/j.neurad.2019.03.001. Epub 2019 Mar 20. J Neuroradiol. 2020. PMID: 30904450 Review.
References
LinkOut - more resources
Full Text Sources
