

Nurse versus doctor management of HIV-infected patients receiving antiretroviral therapy (CIPRA-SA): a randomised non-inferiority trial
- PMID: 20557927
- PMCID: PMC3145152
- DOI: 10.1016/S0140-6736(10)60894-X
Nurse versus doctor management of HIV-infected patients receiving antiretroviral therapy (CIPRA-SA): a randomised non-inferiority trial
Erratum in
- Lancet. 2010 Sep 25;376(9746):1054
Abstract
Background: Expanded access to combination antiretroviral therapy (ART) in resource-poor settings is dependent on task shifting from doctors to other health-care providers. We compared outcomes of nurse versus doctor management of ART care for HIV-infected patients.
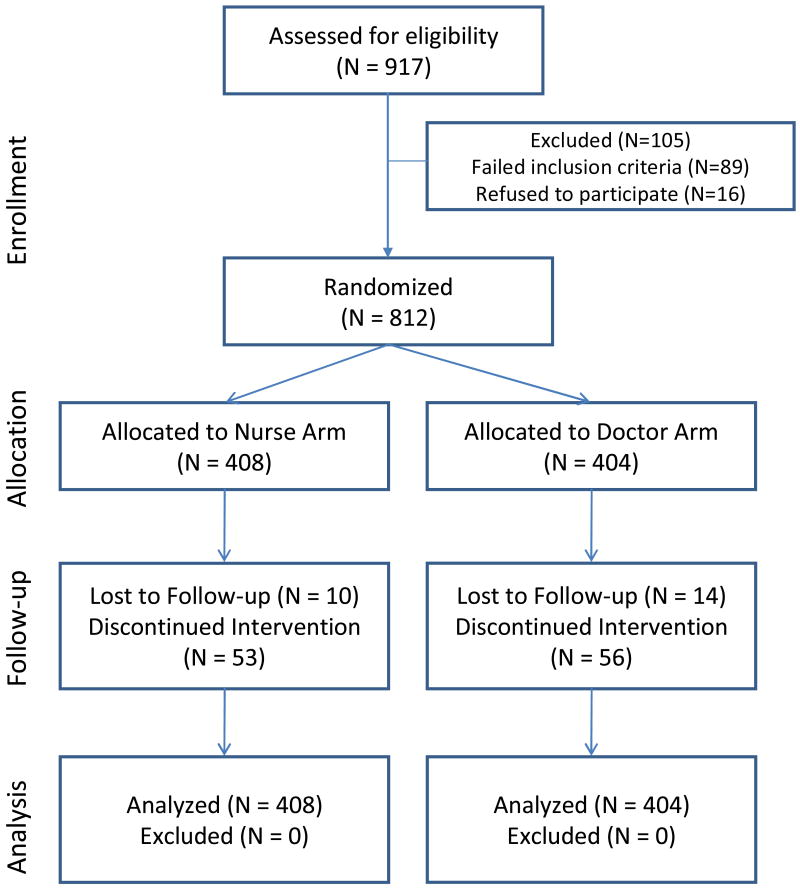
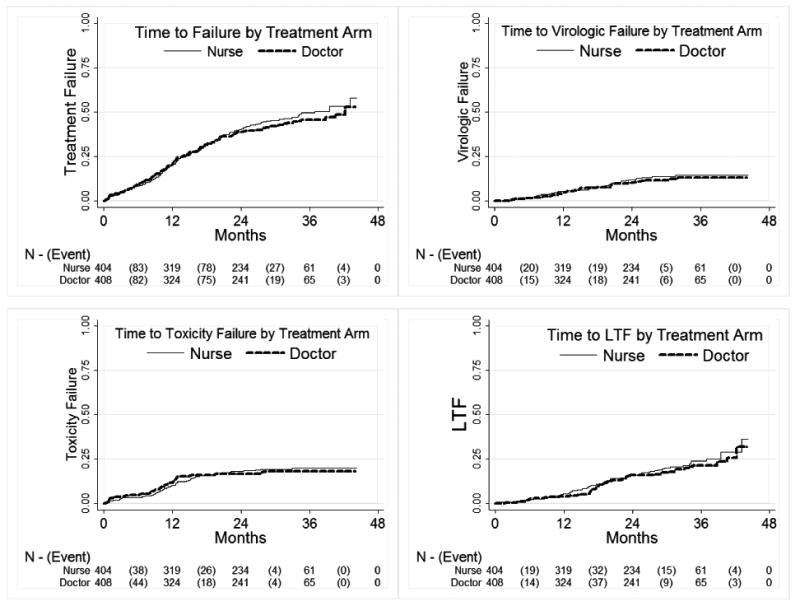
Methods: This randomised non-inferiority trial was undertaken at two South African primary-care clinics. HIV-positive individuals with a CD4 cell count of less than 350 cells per microL or WHO stage 3 or 4 disease were randomly assigned to nurse-monitored or doctor-monitored ART care. Patients were randomly assigned by stratified permuted block randomisation, and neither the patients nor those analysing the data were masked to assignment. The primary objective was a composite endpoint of treatment-limiting events, incorporating mortality, viral failure, treatment-limiting toxic effects, and adherence to visit schedule. Analysis was by intention to treat. Non-inferiority of the nurse versus doctor group for cumulative treatment failure was prespecified as an upper 95% CI for the hazard ratio that was less than 1.40. This study is registered with ClinicalTrials.gov, number NCT00255840.
Findings: 408 patients were assigned to doctor-monitored ART care and 404 to nurse-monitored ART care; all participants were analysed. 371 (46%) patients reached an endpoint of treatment failure: 192 (48%) in the nurse group and 179 (44%) in the doctor group. The hazard ratio for composite failure was 1.09 (95% CI 0.89-1.33), which was within the limits for non-inferiority. After a median follow-up of 120 weeks (IQR 60-144), deaths (ten vs 11), virological failures (44 vs 39), toxicity failures (68 vs 66), and programme losses (70 vs 63) were similar in nurse and doctor groups, respectively.
Interpretation: Nurse-monitored ART is non-inferior to doctor-monitored therapy. Findings from this study lend support to task shifting to appropriately trained nurses for monitoring of ART.
Funding: National Institutes of Health; United States Agency for International Development; National Institute of Allergy and Infectious Diseases.
Copyright 2010 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Operational research in HIV priority areas: the African way.Lancet. 2010 Jul 3;376(9734):4-6. doi: 10.1016/S0140-6736(10)60972-5. Lancet. 2010. PMID: 20557929 No abstract available.
-
Nurse management of HIV-infected patients.Lancet. 2010 Sep 25;376(9746):1053-4. doi: 10.1016/S0140-6736(10)61487-0. Lancet. 2010. PMID: 20870096 No abstract available.
References
-
- Egger M, May M, Chêne G, et al. Prognosis of HIV-1-infected patients starting highly active antiretroviral therapy: a collaborative analysis of prospective studies. The Lancet. 2002;360(9340):1178. - PubMed
-
- Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents. [accessed 25th November 2009];2008 November 3; Available at http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf.
-
- Kitahata MM, Van Rompaey SE, Shields AW. Physician experience in the care of HIV-infected persons is associated with earlier adoption of new antiretroviral therapy. J Acquir Immune Defic Syndr. 2000;24(2):106–14. - PubMed
-
- Landon BE, Wilson IB, McInnes K, et al. Physician specialization and the quality of care for human immunodeficiency virus infection. Arch Intern Med. 2005;165(10):1133–9. - PubMed
-
- Kitahata MM, Koepsell TD, Deyo RA, et al. Physicians' experience with the acquired immunodeficiency syndrome as a factor in patients' survival. N Engl J Med. 1996;334(11):701–6. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
