

Different characteristics of complex fractionated atrial electrograms in acute paroxysmal versus long-standing persistent atrial fibrillation
- PMID: 20558323
- PMCID: PMC4287370
- DOI: 10.1016/j.hrthm.2010.06.018
Different characteristics of complex fractionated atrial electrograms in acute paroxysmal versus long-standing persistent atrial fibrillation
Abstract
Background: Complex fractionated atrial electrograms (CFAEs) may represent a phenomenon associated with sources of atrial fibrillation (AF) and are being used increasingly as targets of catheter ablation. However, current methods have limited efficacy for characterizing CFAEs important to substrate arrhythmogenicity and do not measure electrogram morphology.
Objective: The purpose of this study was to develop a methodology for quantifying the degree of morphologic heterogeneity in CFAE deflections, and to determine whether there are differences in this measurement between paroxysmal and persistent AF patients.
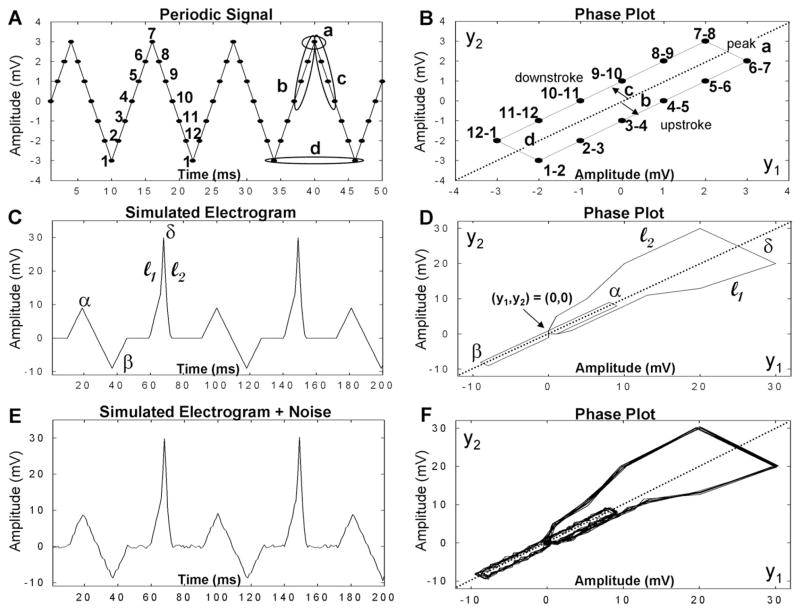
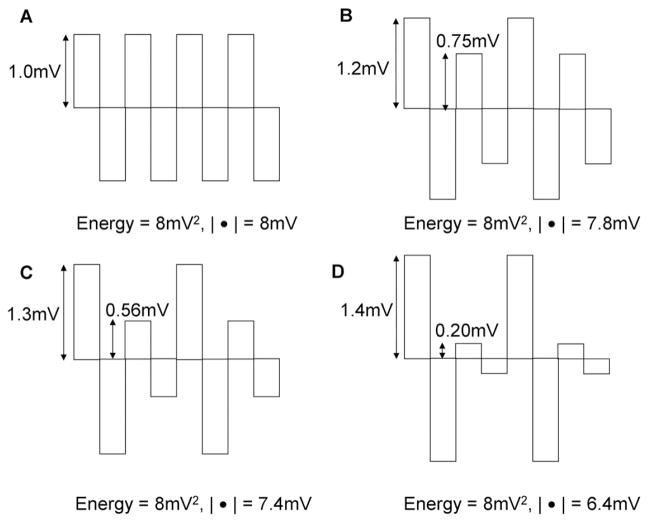
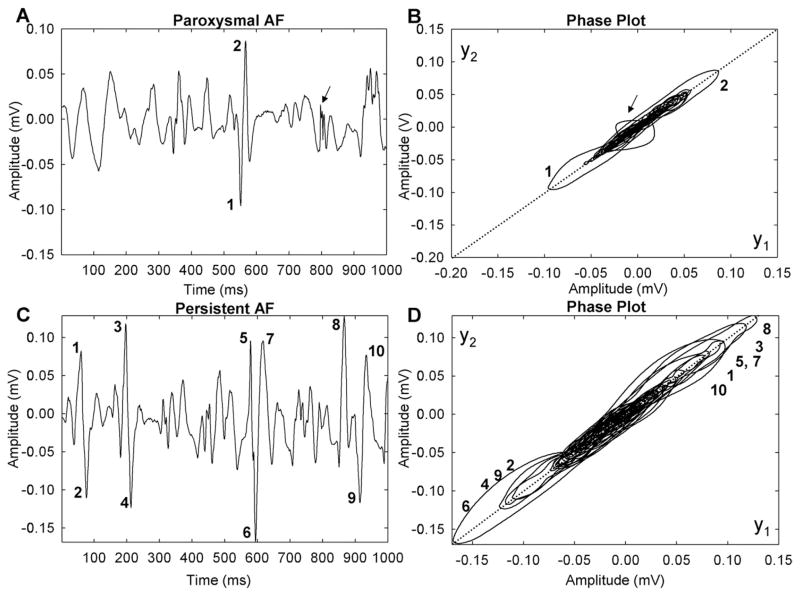
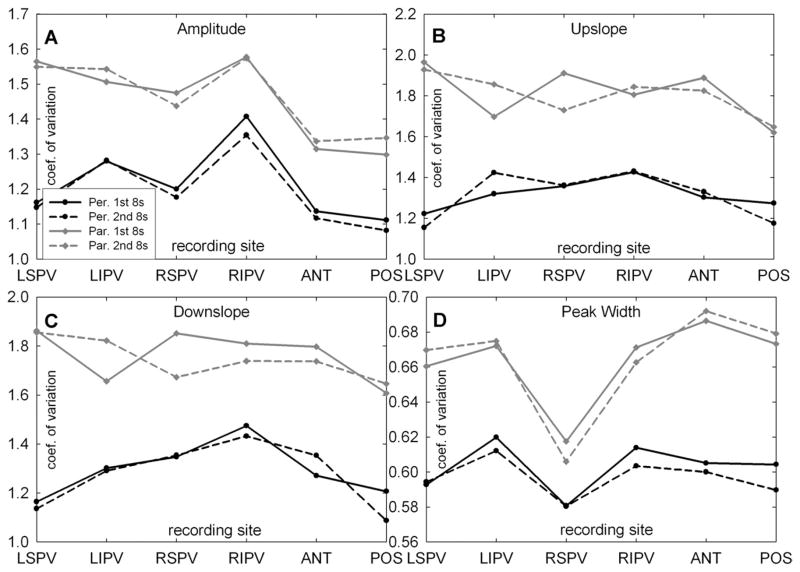
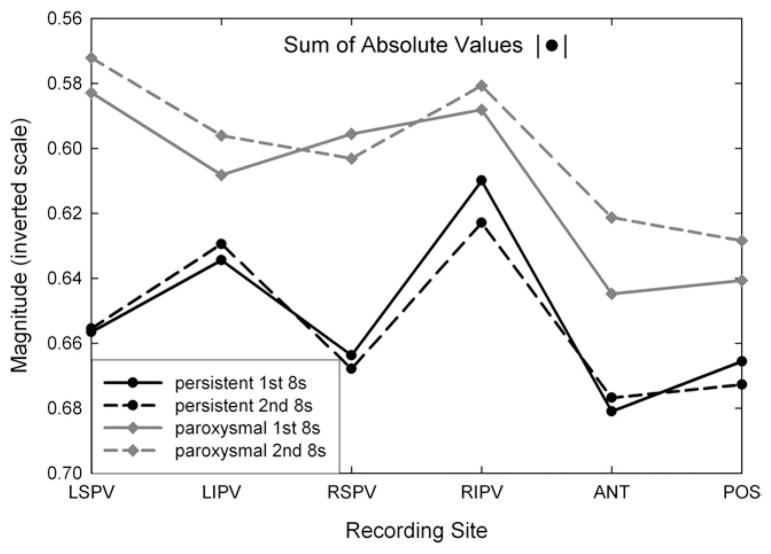
Methods: Two successive bipolar CFAEs of length 8.4 seconds each were acquired during AF from two sites each at the ostia of the four pulmonary veins (PVs) and from the anterior and posterior left atrial free wall in patients with paroxysmal AF (N = 10) and long-standing persistent AF (N = 10). Extrinsic and intrinsic features of electrogram shape were used to characterize fractionation in CFAE sequences. The extrinsic parameters were the amplitude, upslope, downslope, and width of each deflection. The intrinsic parameter was the voltage profile as characterized by the sum of absolute values. These measurements were compared to the mean interval between CFAE deflections, a standard fractionation indicator.
Results: The variability of intrinsic/extrinsic morphologic parameters was higher in paroxysmal than persistent AF at the left superior PV (P < or =.003), the posterior left atrial free wall, anterior left atrial free wall, left inferior PV, and right superior PV (P <.05 for most parameters), and the right inferior PV (not significant). Mean CFAE deflection intervals were longer at all locations in paroxysmal AF but were significant only at the left superior PV and posterior left atrial free wall (P <.05). Quantitative morphologic parameters were not well correlated with dominant frequency (r(2) <0.32); thus, our new measures are robust to changes in activation rate.
Conclusion: A novel method for quantifying CFAEs, independent of activation rate, has been developed. The method demonstrates greater significance in the difference between CFAE morphology in paroxysmal and long-standing AF compared with mean interval between CFAE deflections. The differences identified suggest that CFAE morphology may evolve as AF persists.
Copyright 2010 Heart Rhythm Society. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
The dominant morphology of fractionated atrial electrograms has greater temporal stability in persistent as compared with paroxysmal atrial fibrillation.Comput Biol Med. 2013 Dec;43(12):2127-35. doi: 10.1016/j.compbiomed.2013.08.027. Epub 2013 Oct 10. Comput Biol Med. 2013. PMID: 24290930 Clinical Trial.
-
Differences in repeating patterns of complex fractionated left atrial electrograms in longstanding persistent atrial fibrillation as compared with paroxysmal atrial fibrillation.Circ Arrhythm Electrophysiol. 2011 Aug;4(4):470-7. doi: 10.1161/CIRCEP.110.960153. Epub 2011 May 2. Circ Arrhythm Electrophysiol. 2011. PMID: 21536597 Free PMC article.
-
Spatial relationships between the pulmonary veins and sites of complex fractionated atrial electrograms during atrial fibrillation.Pacing Clin Electrophysiol. 2009 Mar;32 Suppl 1:S190-3. doi: 10.1111/j.1540-8159.2008.02282.x. Pacing Clin Electrophysiol. 2009. PMID: 19250091
-
Pulmonary vein isolation with complex fractionated atrial electrogram ablation for paroxysmal and nonparoxysmal atrial fibrillation: A meta-analysis.Heart Rhythm. 2011 Jul;8(7):994-1000. doi: 10.1016/j.hrthm.2011.02.033. Epub 2011 Mar 10. Heart Rhythm. 2011. PMID: 21397045 Free PMC article. Review.
-
Additional complex fractionated atrial electrogram ablation does not improve the outcomes of non-paroxysmal atrial fibrillation: A systematic review and meta-analysis of randomized controlled trials.Indian Heart J. 2021 Jan-Feb;73(1):63-73. doi: 10.1016/j.ihj.2020.11.004. Epub 2020 Nov 7. Indian Heart J. 2021. PMID: 33714411 Free PMC article.
Cited by
-
Practical Considerations for the Application of Nonlinear Indices Characterizing the Atrial Substrate in Atrial Fibrillation.Entropy (Basel). 2022 Sep 8;24(9):1261. doi: 10.3390/e24091261. Entropy (Basel). 2022. PMID: 36141147 Free PMC article.
-
Ablation of Longstanding Persistent Atrial Fibrillation.J Atr Fibrillation. 2010 Oct 22;3(3):321. doi: 10.4022/jafib.321. eCollection 2010 Oct-Nov. J Atr Fibrillation. 2010. PMID: 28496676 Free PMC article. Review. No abstract available.
-
Effect of Pulmonary Vein Isolation with Left Atrial Wall Isolation Plus Selective CFAE Ablation in Patients with Persistent Atrial Fibrillation.J Cardiovasc Dev Dis. 2024 Oct 4;11(10):308. doi: 10.3390/jcdd11100308. J Cardiovasc Dev Dis. 2024. PMID: 39452279 Free PMC article.
-
Complex fractionated atrial electrograms: is this the beast to tame in atrial fibrillation?Circ Arrhythm Electrophysiol. 2011 Aug;4(4):426-8. doi: 10.1161/CIRCEP.111.964841. Circ Arrhythm Electrophysiol. 2011. PMID: 21846887 Free PMC article. No abstract available.
-
Spectral profiles of complex fractionated atrial electrograms are different in longstanding and acute onset atrial fibrillation atrial electrogram spectra.J Cardiovasc Electrophysiol. 2012 Sep;23(9):971-9. doi: 10.1111/j.1540-8167.2012.02349.x. Epub 2012 May 11. J Cardiovasc Electrophysiol. 2012. PMID: 22578068 Free PMC article.
References
-
- Stiles MK, Brooks AG, Sanders P. Putting CFAE on the map. J Cardiovasc Electrophysiol. 2008;19:904–906. - PubMed
-
- Nademanee K, McKenzie J, Kosar E, et al. A new approach for catheter ablation of atrial fibrillation: mapping of the electrophysiologic substrate. J Am Coll Cardiol. 2004;43:2044–2053. - PubMed
-
- Porter M, Spear W, Akar JG, et al. Prospective study of atrial fibrillation termination during ablation guided by automated detection of fractionated electrograms. J Cardiovasc Electrophysiol. 2008;19:613–620. - PubMed
-
- Jaïs P, Haïssaguerre M, Shah DC, Chouairi S, Clémenty J. Regional disparities of endocardial atrial activation in paroxysmal atrial fibrillation. Pacing Clin Electrophysiol. 1996;11(Pt 2):1998–2003. - PubMed
-
- Widrow B. Rubber-mask technique 1. Pattern measurement and analysis. Pattern Recognit. 1973;5:175–197.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
