

Relationship between inpatient hyperglycemia and insulin treatment after kidney transplantation and future new onset diabetes mellitus
- PMID: 20558559
- PMCID: PMC2974410
- DOI: 10.2215/CJN.09481209
Relationship between inpatient hyperglycemia and insulin treatment after kidney transplantation and future new onset diabetes mellitus
Abstract
Background and objectives: Approximately two-thirds of kidney transplant recipients with no previous history of diabetes experience inpatient hyperglycemia immediately after kidney transplant surgery; whether inpatient hyperglycemia predicts future new onset diabetes after transplant (NODAT) is not established.
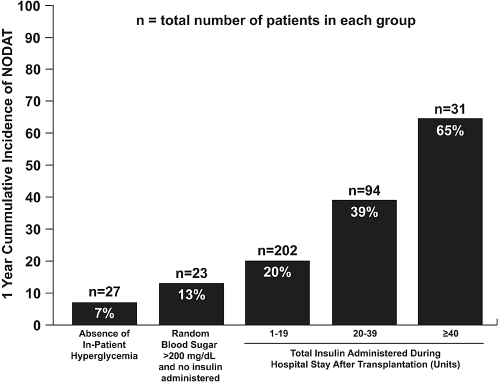
Design, setting, participants, & measurements: A retrospective study was conducted to determine the risk conferred by inpatient hyperglycemia on development of NODAT within 1 year posttransplant. All adult nondiabetic kidney transplant recipients between June 1999 and January 2008 were included. Posttransplant inpatient hyperglycemia was defined as any bedside capillary blood glucose > or = 200 mg/dl or insulin therapy during hospitalization. NODAT was defined as HbA1C > or = 6.5%, fasting venous serum glucose > or = 126 mg/dl, or prescribed diet or medical therapy for diabetes mellitus.
Results: The study cohort included 377 patients. NODAT developed in 1 (4%) of the 28 patients without inpatient hyperglycemia, 4 (18%) of the 22 patients with inpatient hyperglycemia but not treated with insulin, and in 98 (30%) of the 327 of the patients who were diagnosed with inpatient hyperglycemia and were treated with insulin. In adjusted analyses, requirement of insulin therapy during hospitalization posttransplant was associated with a 4-fold increase in NODAT (relative risk 4.01; confidence interval, 1.49 to 10.7; P = 0.006).
Conclusion: Development of inpatient hyperglycemia after kidney transplantation in nondiabetic patients significantly increased the risk of NODAT. Additionally, we observed a significantly increased risk of cardiovascular events in patients who developed NODAT.
Figures
References
-
- Cosio FG, Pesavento TE, Kim S, Osei K, Henry M, Ferguson RM: Patient survival after renal transplantation: IV. Impact of post-transplant diabetes. Kidney Int 62: 1440–1446, 2002 - PubMed
-
- Kasiske BL, Snyder JJ, Gilbertson D, Matas AJ: Diabetes mellitus after kidney transplantation in the United States. Am J Transplant 3: 178–185, 2003 - PubMed
-
- Nam JH, Mun JI, Kim SI, Kang SW, Choi KH, Park K, Ahn CW, Cha BS, Song YD, Lim SK, Kim KR, Lee HC, Huh KB: Beta-Cell dysfunction rather than insulin resistance is the main contributing factor for the development of postrenal transplantation diabetes mellitus. Transplantation 71: 1417–1423, 2001 - PubMed
-
- Woodward RS, Schnitzler MA, Baty J, Lowell JA, Lopez-Rocafort L, Haider S, Woodworth TG, Brennan DC: Incidence and cost of new onset diabetes mellitus among U.S. wait-listed and transplanted renal allograft recipients. Am J Transplant 3: 590–598, 2003 - PubMed
-
- Ducloux D, Kazory A, Chalopin JM: Posttransplant diabetes mellitus and atherosclerotic events in renal transplant recipients: A prospective study. Transplantation 79: 438–443, 2005 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
