

Continuous renal replacement therapy may increase the risk of catheter infection
- PMID: 20558562
- PMCID: PMC2924410
- DOI: 10.2215/CJN.02130310
Continuous renal replacement therapy may increase the risk of catheter infection
Abstract
Background and objectives: Little is known about the risks of catheter-related infections in patients undergoing intermittent hemodialysis (IHD) as compared with continuous renal replacement therapy (CRRT) techniques. We compared the two modalities among critically ill adults requiring acute renal replacement therapy (RRT).
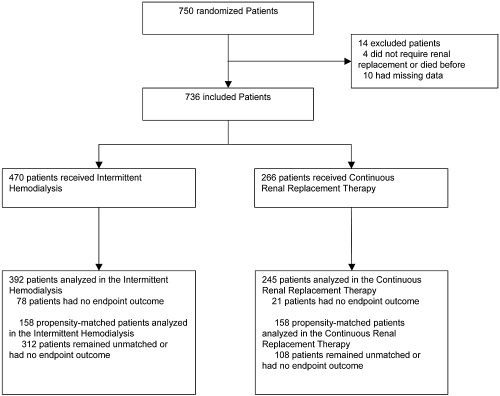
Design, setting, participants, & measurements: We used the multicenter Cathedia study cohort of 736 critically ill adults requiring RRT. Cox marginal structural models were used to compare time to catheter-tip colonization at removal (intent-to-treat, primary endpoint) among patients who started IHD (n = 470) versus CRRT (n = 266). On-treatment analysis was also conducted to take into account changes in prescription of RRT modality.
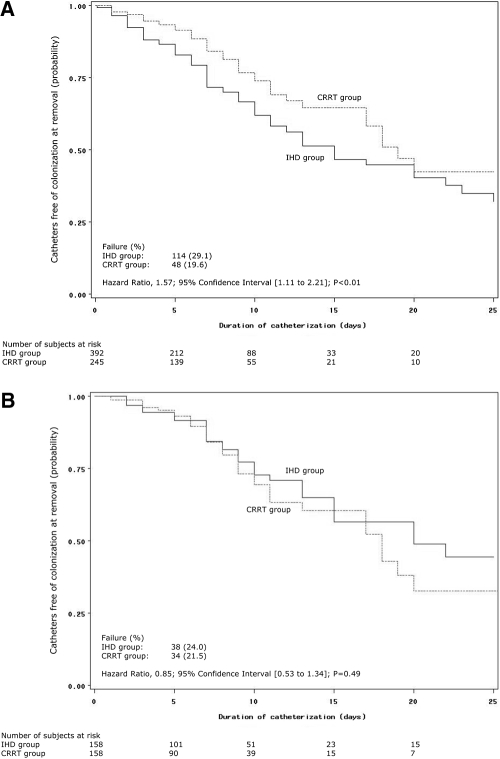
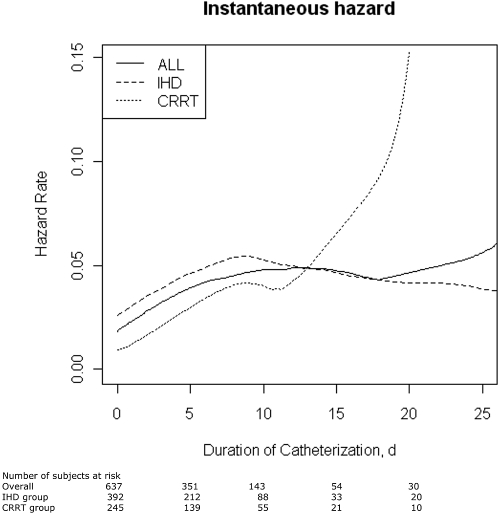
Results: Hazard rate of catheter-tip colonization did not increase within the first 10 days of catheter use. Predictors of catheter-tip colonization were higher lactate levels and hypertension, while systemic antibiotics, antiseptics-impregnated catheters, and mechanical ventilation were associated with decreased risk. The incidence of catheter-tip colonization per 1000 catheter-days was 42.7 in the IHD group and 27.7 in the CRRT group (P < 0.01). This association was no longer significant after correction for channeling bias (weighted HR, 0.96; 95% CI: 0.77 to 1.20, P = 0.73). On-treatment analysis revealed an increased risk of primary endpoint during CRRT exposure as compared with IHD exposure (weighted HR, 0.71; 95% CI: 0.56 to 0.92, P < 0.009).
Conclusions: Our results do not support the use of CRRT when IHD could be an alternative to reduce the risk of catheter-related infection.
Figures
References
-
- Mermel LA: Prevention of intravascular catheter-related infections. Ann Intern Med 132: 391–402, 2000 - PubMed
-
- Hoste EA, Blot SI, Lameire NH, Vanholder RC, De Bacquer D, Colardyn FA: Effect of nosocomial bloodstream infection on the outcome of critically ill patients with acute renal failure treated with renal replacement therapy. J Am Soc Nephrol 15: 454–462, 2004 - PubMed
-
- Reynvoet E, Vandijck DM, Blot SI, Dhondt AW, De Waele JJ, Claus S, Buyle FM, Vanholder RC, Hoste EA: Epidemiology of infection in critically ill patients with acute renal failure. Crit Care Med 37: 2203–2209, 2009 - PubMed
-
- Rabindranath K, Adams J, Macleod AM, Muirhead N: Intermittent versus continuous renal replacement therapy for acute renal failure in adults. Cochrane Database Syst Rev 3: CD003773, 2007 - PubMed
-
- Randolph AG, Cook DJ, Gonzales CA, Andrew M: Benefit of heparin in central venous and pulmonary artery catheters: A meta-analysis of randomized controlled trials. Chest 113: 165–171, 1998 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
