

Cutaneous vascular and sudomotor responses in human skin grafts
- PMID: 20558761
- PMCID: PMC2980376
- DOI: 10.1152/japplphysiol.00466.2010
Cutaneous vascular and sudomotor responses in human skin grafts
Abstract
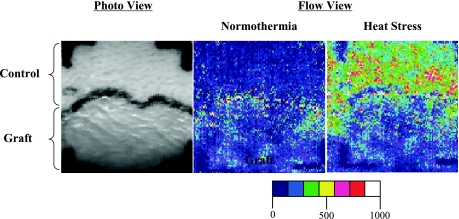
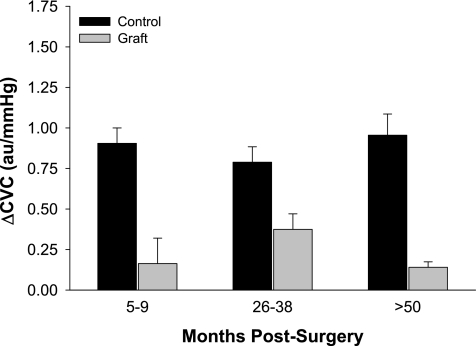
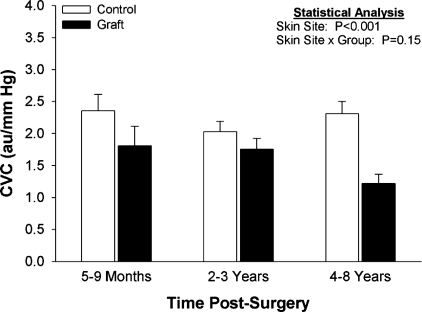
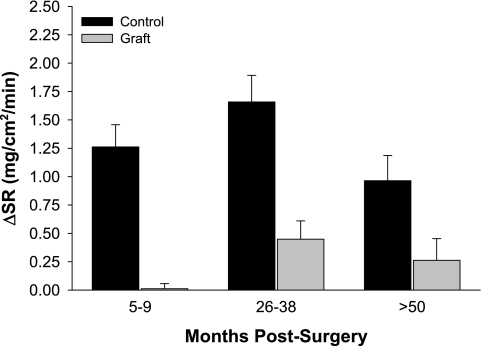
Each year millions of individuals sustain burns. Within the US 40,000-70,000 individuals are hospitalized for burn-related injuries, some of which are quite severe, requiring skin grafting. The grafting procedure disrupts neural and vascular connections between the host site and the graft, both of which are necessary for that region of skin to contribute to temperature regulation. With the use of relatively modern techniques such as laser-Doppler flowmetry and intradermal microdialysis, a wealth of information has become available regarding the consequences of skin grafting on heat dissipation and heat conservation mechanisms. The prevailing data suggest that cutaneous vasodilator capacity to an indirect heat stress (i.e., heating the individual but not the evaluated graft area) and a local heating stimulus (i.e., directly heating the graft area) is impaired in grafted skin. These impairments persist for ≥4 yr following the grafting procedures and are perhaps permanent. The capacity for grafted skin to vasodilate to an endothelial-dependent vasodilator is likewise impaired, whereas its capacity to vasodilate to an endothelial-independent vasodilator is generally preserved. Sweating responsiveness is minimal to nonexistent in grafted skin to both a whole body heat stress and local administration of the primary neurotransmitter responsible for stimulating sweat glands (i.e., acetylcholine). Likewise, there is no evidence that this absence of sweat gland responsiveness improves as the graft matures. In contrast to the heating stimuli, cutaneous vasoconstrictor responses to both indirect whole body cooling (i.e., exposing the individual to a cold stress but not at the evaluated graft area) and direct local cooling (i.e., directly cooling the graft area) are preserved in grafted skin as early as 5-9 mo postgrafting. If uninjured skin does not compensate for impaired heat dissipation of grafted skin, individuals having skin grafts encompassing significant fractions of their body surface area will be at a greater risk for a hyperthermic-related injury. Conversely, the prevailing data suggest that such individuals will not be at a greater risk of hypothermia upon exposure to cold environmental conditions.
Figures


References
-
- Ablove RH, Howell RM. The physiology and technique of skin grafting. Hand Clin 13: 163–173, 1997 - PubMed
-
- American Burn Association American Burn Association National Burn Repository (2006 Report). Chicago, IL: American Burn Association, 2007
-
- Anonymous Ambulatory and Inpatient Procedures in the United States, 1996. Washington, DC: Center for Disease Control and Prevention, 1998
-
- Austin KG, Hansbrough JF, Dore C, Noordenbos J, Buono MJ. Thermoregulation in burn patients during exercise. J Burn Care Rehabil 24: 9–14, 2003 - PubMed
-
- Ben-Simchon C, Tsur H, Keren G, Epstein Y, Shapiro Y. Heat tolerance in patients with extensive healed burns. Plast Reconstr Surg 67: 499–504, 1981 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical