

An ounce of prevention is worth a pound of cure: a cost-effectiveness analysis of incidentally detected aneurysms in functional MRI research
- PMID: 20561317
- PMCID: PMC10517630
- DOI: 10.1111/j.1524-4733.2010.00755.x
An ounce of prevention is worth a pound of cure: a cost-effectiveness analysis of incidentally detected aneurysms in functional MRI research
Abstract
Purpose: Despite ongoing debate about best practices for managing incidentally detected findings in brain research studies using magnetic resonance imaging (MRI), this issue has not been investigated from a health economics viewpoint. We applied a decision-analytic approach to assess the benefit of various strategies for functional MRI (fMRI) studies using intracranial aneurysms (IA) as a model.
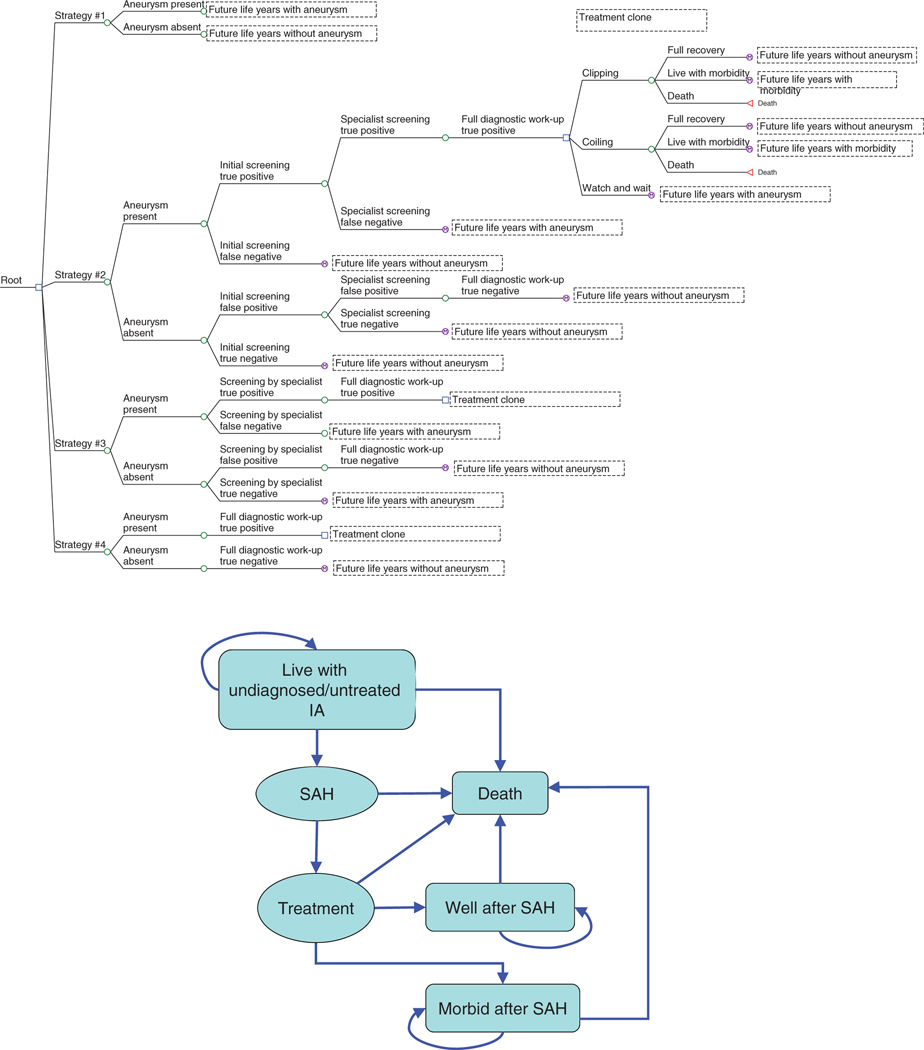
Methods: A decision tree and Markov model were created to simulate the impact on the lifetime costs and quality-adjusted life-years (QALY) of four different strategies for review of scans for the presence of IA. To populate the decision model, we used current evidence from the literature and results from a survey of experts.
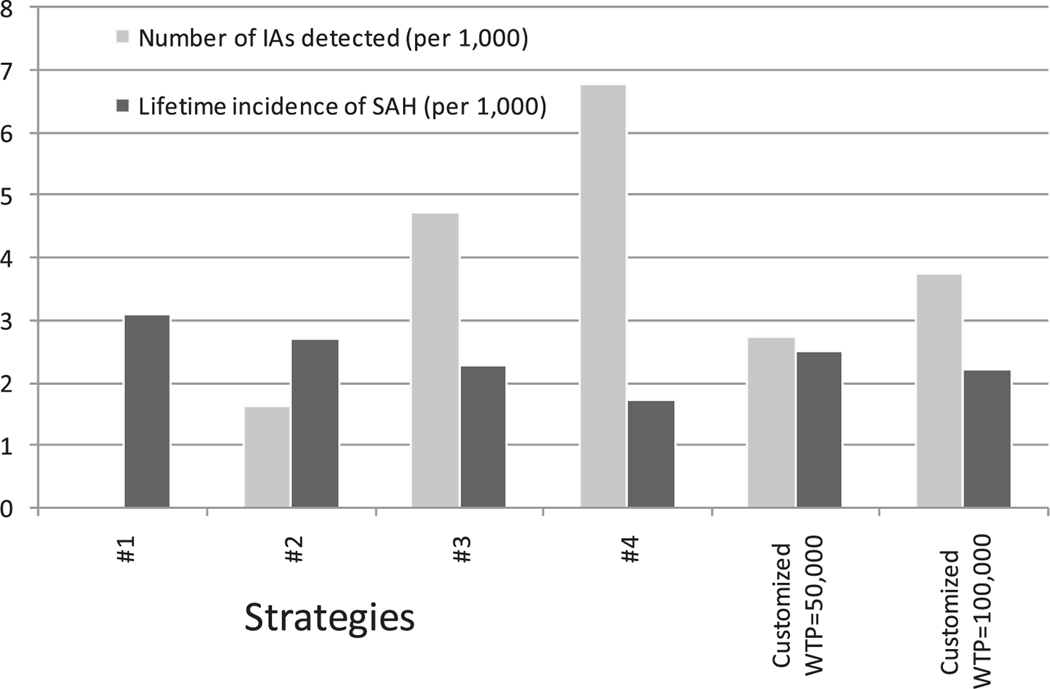
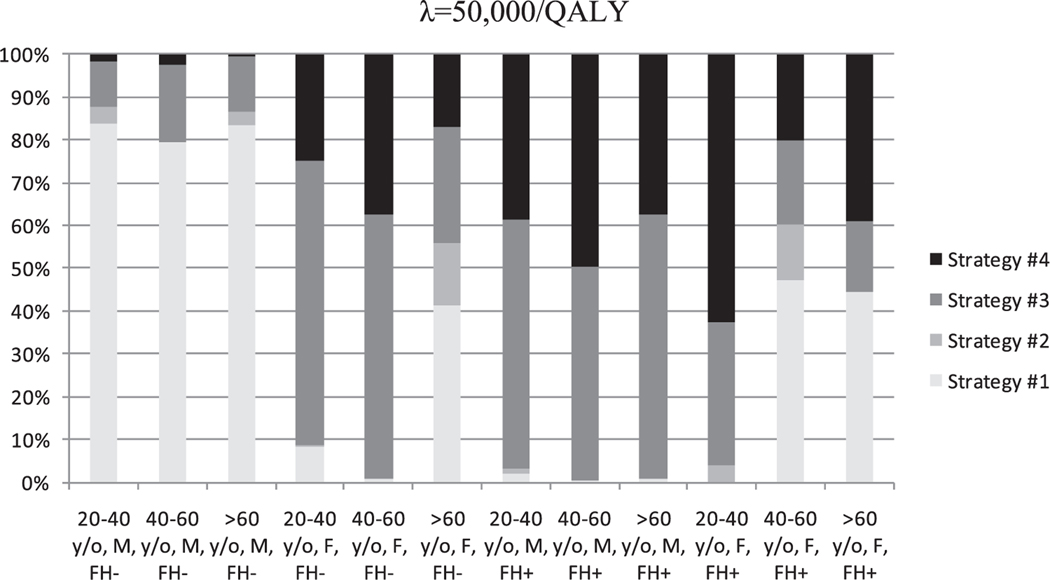
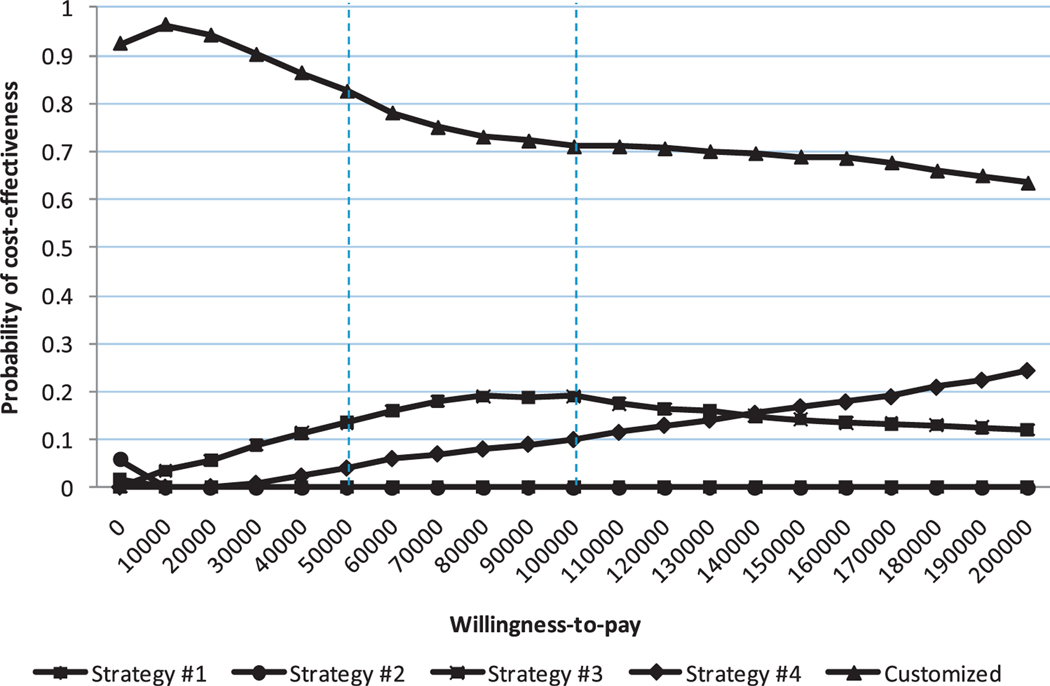
Results: Review of the anatomical scans by a nonspecialist is not cost-effective in any of the subgroups of participants. Full clinical examination of women with a positive family history before enrollment in a study is cost-effective. Cost-effectiveness of reviewing scans obtained from women without a family history and men with a positive family history of IA depends on the willingness-to-pay (λ) for a QALY: at λ of $50,000/QALY, review of scans by a specialist is cost-effective, whereas at λ of $100,000/QALY, a full clinical workup is the best option. Compared with not reviewing any scans, a customized strategy for each subgroup of participants results in an incremental cost-effectiveness ratio of $12,503 for λ=$50,000/QALY and $32,767 for λ=$100,000/QALY.
Conclusion: Tailored strategies based on the characteristics of research participants and λ for one QALY are needed to address the problem of incidental findings in research fMRI studies.
© 2010, International Society for Pharmacoeconomics and Outcomes Research (ISPOR).
Figures
Similar articles
-
Cost-effectiveness of magnetic resonance angiography versus intra-arterial digital subtraction angiography to follow-up patients with coiled intracranial aneurysms.Stroke. 2010 Aug;41(8):1736-42. doi: 10.1161/STROKEAHA.110.585083. Epub 2010 Jul 1. Stroke. 2010. PMID: 20595661
-
Artificial intelligence support in MR imaging of incidental renal masses: an early health technology assessment.Eur Radiol. 2024 Sep;34(9):5856-5865. doi: 10.1007/s00330-024-10643-5. Epub 2024 Feb 23. Eur Radiol. 2024. PMID: 38388721 Free PMC article.
-
Cost-effectiveness of magnetic resonance (MR) imaging and MR-guided targeted biopsy versus systematic transrectal ultrasound-guided biopsy in diagnosing prostate cancer: a modelling study from a health care perspective.Eur Urol. 2014 Sep;66(3):430-6. doi: 10.1016/j.eururo.2013.12.012. Epub 2013 Dec 21. Eur Urol. 2014. PMID: 24377803
-
Screening individuals with intracranial aneurysms for abdominal aortic aneurysms is cost-effective based on estimated coprevalence.J Vasc Surg. 2016 Sep;64(3):811-818.e3. doi: 10.1016/j.jvs.2016.05.065. J Vasc Surg. 2016. PMID: 27565600 Review.
-
Multi-gene Pharmacogenomic Testing That Includes Decision-Support Tools to Guide Medication Selection for Major Depression: A Health Technology Assessment.Ont Health Technol Assess Ser. 2021 Aug 12;21(13):1-214. eCollection 2021. Ont Health Technol Assess Ser. 2021. PMID: 34484487 Free PMC article.
Cited by
-
Incidental Intracranial Findings and Their Clinical Impact; The HUNT MRI Study in a General Population of 1006 Participants between 50-66 Years.PLoS One. 2016 Mar 7;11(3):e0151080. doi: 10.1371/journal.pone.0151080. eCollection 2016. PLoS One. 2016. PMID: 26950220 Free PMC article.
-
Far from Home: Managing Incidental Findings in Field Research with Portable MRI.J Law Med Ethics. 2024;52(4):805-815. doi: 10.1017/jme.2024.169. Epub 2025 Jan 31. J Law Med Ethics. 2024. PMID: 39885754 Free PMC article.
-
Disclosing pathogenic genetic variants to research participants: quantifying an emerging ethical responsibility.Genome Res. 2012 Mar;22(3):421-8. doi: 10.1101/gr.127845.111. Epub 2012 Jan 6. Genome Res. 2012. PMID: 22147367 Free PMC article.
-
Brain imaging: incidental findings: in practice and in person.Nat Rev Neurol. 2009 Dec;5(12):643-4. doi: 10.1038/nrneurol.2009.192. Nat Rev Neurol. 2009. PMID: 19953113 Free PMC article.
-
Incidental findings in neuroimaging research: a framework for anticipating the next frontier.J Empir Res Hum Res Ethics. 2012 Feb;7(1):53-7. doi: 10.1525/jer.2012.7.1.53. J Empir Res Hum Res Ethics. 2012. PMID: 22378134 Free PMC article.
References
-
- Katzman GL, Dagher AP, Patronas NJ. Incidental findings on brain magnetic resonance imaging from 1000 asymptomatic volunteers. JAMA 1999;282:36–9. - PubMed
-
- Illes J, Desmond JE, Huang LF, et al. Ethical and practical considerations in managing incidental findings in functional magnetic resonance imaging. Brain Cogn 2002;50:358–65. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
