

Prenatal diagnosis and risk factors for preoperative death in neonates with single right ventricle and systemic outflow obstruction: screening data from the Pediatric Heart Network Single Ventricle Reconstruction Trial(∗)
- PMID: 20561642
- PMCID: PMC3143839
- DOI: 10.1016/j.jtcvs.2010.05.022
Prenatal diagnosis and risk factors for preoperative death in neonates with single right ventricle and systemic outflow obstruction: screening data from the Pediatric Heart Network Single Ventricle Reconstruction Trial(∗)
Abstract
Objectives: The purpose of this analysis was to assess preoperative risk factors before the first-stage Norwood procedure in infants with hypoplastic left heart syndrome and related single-ventricle lesions and to evaluate practice patterns in prenatal diagnosis, as well as the role of prenatal diagnosis in outcome.
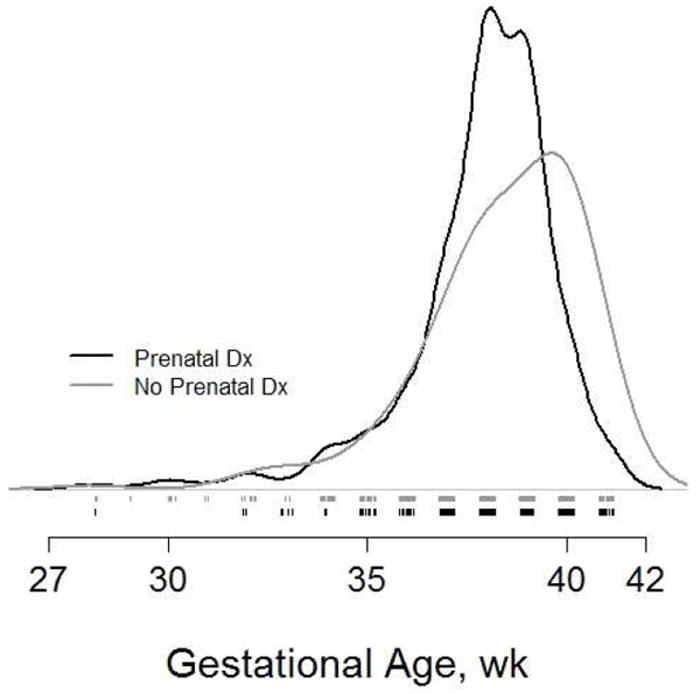
Methods: Data from all live births with morphologic single right ventricle and systemic outflow obstruction screened for the Pediatric Heart Network's Single Ventricle Reconstruction Trial were used to investigate prenatal diagnosis and preoperative risk factors. Demographics, gestational age, prenatal diagnosis status, presence of major extracardiac congenital abnormalities, and preoperative mortality rates were recorded.
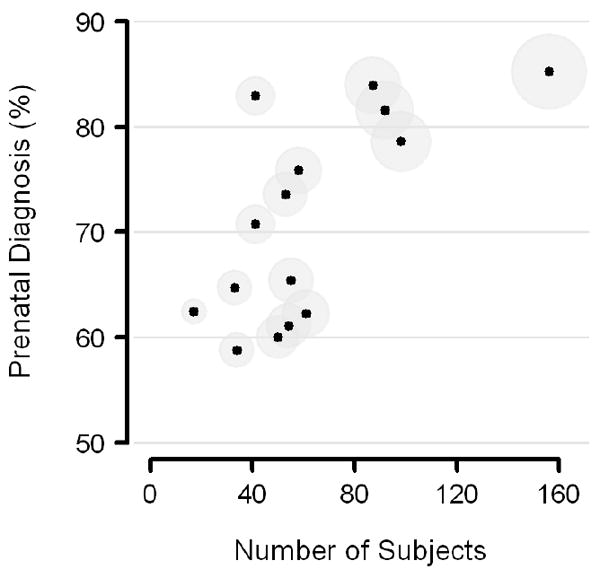
Results: Of 906 infants, 677 (75%) had prenatal diagnosis, 15% were preterm (<37 weeks' gestation), and 16% were low birth weight (<2500 g). Rates of prenatal diagnosis varied by study site (59% to 85%, P < .0001). Major extracardiac congenital abnormalities were less prevalent in those born after prenatal diagnosis (6% vs 10%, P = .03). There were 26 (3%) deaths before Norwood palliation; preoperative mortality did not differ by prenatal diagnosis status (P = .49). In multiple logistic regression models, preterm birth (P = .02), major extracardiac congenital abnormalities (P < .0001), and obstructed pulmonary venous return (P = .02) were independently associated with preoperative mortality.
Conclusions: Prenatal diagnosis occurred in 75%. Preoperative death was independently associated with preterm birth, obstructed pulmonary venous return, and major extracardiac congenital abnormalities. Adjusted for gestational age and the presence of obstructed pulmonary venous return, the estimated odds of preoperative mortality were 10 times greater for subjects with a major extracardiac congenital abnormality.
Copyright © 2010 The American Association for Thoracic Surgery. All rights reserved.
Figures
References
-
- Chang RK, Chen AY, Klitzner TS. Clinical management of infants with hypoplastic left heart syndrome in the United States, 1988-1997. Pediatrics. 2002 Aug;110(2 Pt 1):292–8. - PubMed
-
- Rasiah SV, Ewer AK, Miller P, Wright JG, Barron DJ, Brawn WJ, et al. Antenatal perspective of hypoplastic left heart syndrome: 5 years on. Arch Dis Child Fetal Neonatal Ed. 2008 May;93(3):F192–F197. - PubMed
-
- Allan LD, Sharland GK, Milburn A, Lockhart SM, Groves AM, Anderson RH, et al. Prospective diagnosis of 1,006 consecutive cases of congenital heart disease in the fetus. J Am Coll Cardiol. 1994 May;23(6):1452–8. - PubMed
-
- Kumar RK, Newburger JW, Gauvreau K, Kamenir SA, Hornberger LK. Comparison of outcome when hypoplastic left heart syndrome and transposition of the great arteries are diagnosed prenatally versus when diagnosis of these two conditions is made only postnatally. Am J Cardiol. 1999 Jun 15;83(12):1649–53. - PubMed
